Notes on clinical predictions to distinguish pelvic inflammatory disease
•Télécharger en tant que DOC, PDF•
1 j'aime•533 vues

appendicitis vs PID

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
Similaire à Notes on clinical predictions to distinguish pelvic inflammatory disease
Similaire à Notes on clinical predictions to distinguish pelvic inflammatory disease (20)
Plus de Tana Kiak
Dernier
Dernier (20)
Notes on clinical predictions to distinguish pelvic inflammatory disease
- 1. NOTES ON CLNICAL PREDICTORS TO DISTINGUISH PELVIC INFLAMMATORY DISEASE FROM APPENDICITIS PREPARED BY DR.KIAK-2014
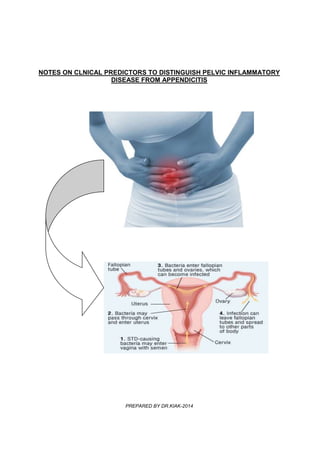
- 2. MISDIAGNOSIS IN WOMEN OF CHILDBEARING AGE BACKGROUND Diagnosis of the cause of lower abdominal pain in women may be difficult because appendicitis and pelvic inflammatory disease often present similarly. Although no single finding can define the diagnosis, the history and physical findings reported herein provide a number of criteria which, when taken together, will usually allow a confident diagnosis of either appendicitis or pelvic inflammatory disease to be made. Attention to these items can improve precision in diagnosis and lessen the incidence of unnecessary laparotomy, which carries a well-documented complication rate of 10 to 20 percent. CLINICAL PREDICTIONS TO DISTINGUISH PELVIC INFLAMMATORY DISEASE & APPENDICITIS - Appendicitis and Pelvic Inflammatory Disease (PID) are the most common causes of abdominal pain in women in childbearing age. - Due to the similar presentations of the conditions, the rate of misdiagnosis is high - - American College Emergency Physicians reports that up to one third (33%) of women of childbearing age with appendicitis are misdiagnosed. - The most common misdiagnosis are PID and STI - Literature shows 20% - 30% a false positive appendectomy rate in men is almost twice as high in women. Sequelae of Untreated Appendicitis or PID - A delay lack of treatment for Acute appendicitis usually results in appendix perforation. - Delay treatment of PID also has severe consequences. Sequelae of untreated PID can include increased risk of o Ectopic pregnancy o Infertility o Pyosalpinx o Chronic pelvic pain o Dyspareunia o Tubo-ovarian abscess o Recurrent PID - Early evaluation strategies in diagnosis both conditions are helpful that can minimize mortality and morbidity Clinical Manifestations - Appendicitis is defined as an inflammation of the inner lining of the vermiform appendix that spreads to its other parts., caused by a variety of mechanisms. o It starts as a referred pain due to inflammation that gradually localizes to the RLQ of the abdomen o Due to inflammation and reduced blood supply to the appendix, infarction occurs, gangrene & perforation ensure within 24-36hrs - Classic symptoms o Migration of pain from mid-abdomen to RLQ (McBurney’s point) o Nausea & Vomiting o Anorea & Low-Grade fever Note: 50% do not present with above symptoms - PID is an infection that involves o Uterus o Fallopian tubes
- 3. o Adjacent pelvic structures (endometritsi, parametritis, oophoritis, salpingitis, TOA, peritonitis) Common cuases are due to Neisseria gonorrhea or Chlamydia trachomatis) - Differentiating Data o Literature focuses on diagnostic techniques that have no proven useful in differentiating acute appendicitis from PID o Some assessments are part of a thorough exam & may assist in diffentiating the two conditions o The level of urinary beta–human chorionic gonadotropin (beta-hCG) is useful in differentiating appendicitis from early ectopic pregnancy. However, with regard to the WBC count, physiologic leukocytosis during pregnancy makes this study less useful in the diagnosis than at other times, and no reliable distinguishing WBC parameters are cited in the literature. Pelvic Inflammatory Disease - Purulent cervical discharge - Lab evidence of gonorrhea or Chlamydia infection - History of PID or other STI - Ages 15-24 years old - Multiple sexual partners - No use of Contraceptives - Presence of pain during 1st 7days of menstrual cycle - No relief of pain with change of body position - Re-current pain - 10 or more PMS on G-stain of endocervical cells - positive urinalysis APPENDICITIS - Migrating pain from mid-abdomen to RLQ – periumbilical pain - Nausea 61-92% - Vomiting; Nearly always follows the onset of pain - Anorexia 74 – 78% - Diarrhea or constipation: as many as 18 % of patients - Positive family history of Appendicitis - Some relief of pain with body positioning - Pain less than 2-3 days - Only one current episode of pain Not useful in differentiating btw PID & APPPENDICITIS - Cervical motion tenderness - Erythrocyte sedimentation rate (ESR) - C-reactive protein - Rovsing, psoas & Obturatory signs - Plain Radiograph - Digital Rectal Examination - Bowel sounds REFERENCE http://emedicine.medscape.com/article/773895-differential