Dengue Fever: A Guide
•Télécharger en tant que PPTX, PDF•
49 j'aime•5,399 vues

This presentation gives a vivid description about dengue fever.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (20)
Similaire à Dengue Fever: A Guide
Similaire à Dengue Fever: A Guide (20)
Dernier
Dernier (20)
Dengue Fever: A Guide
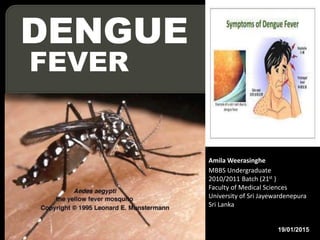
- 1. DENGUE FEVER Amila Weerasinghe MBBS Undergraduate 2010/2011 Batch (21st ) Faculty of Medical Sciences University of Sri Jayewardenepura Sri Lanka 19/01/2015
- 2. 1. What is ‘’Dengue’’ ? 2. Epidemiology 3. Vector 4. Virus 5. Pathogenesis of the disease 6. Classification 7. The natural course of the illness 8. Diagnosis and Management at OPD level and by primary care physician. 9. In-ward Management of DF/DHF 10. Management of complicated patients Contents
- 3. A vector borne disease. The most rapidly spreading mosquito- borne viral disease in the world. A notificable disease in Sri Lanka
- 4. World situation last 50 years, 30 fold rise 2.5 billion or 40% of the world, live in dengue endemic countries. WHO (2009).Dengue: guidelines for diagnosis, treatment, prevention and control -- New edition
- 5. Yearly 50 to 100 million infections 500,000 DHF cases 22,000 deaths, mostly among children.
- 7. Sri Lankan situation First serologically confirmed case - 1962 First documented dengue outbreak - 1965- 1966 First epidemic of DHF/ Dengue Shock Syndrome - 1989 – 1990.
- 8. 2014 46584
- 9. 0 5000 10000 15000 20000 25000 30000 35000 40000 45000 50000 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 Cases
- 10. Year 2014, 46584 suspected dengue cases 55.26% of dengue cases from the Western province. http://www.epid.gov.lk http://www.dengue.health.gov.lk
- 13. A biological vector – Mosquitoes In Sri Lanka Aedes albopictus and Aedes aegypti Aedes aegypti is the main species.
- 14. Genus – Flavi virus Family – Flaviviridae Virus – Dengue virus (DEN) Serotypes – 4 serotypes DEN 1 to 4
- 15. Primary dengue infection First time viral infection, Any of the 4 virus types .
- 16. Secondary dengue infection # Viral infection, except which resulted the primary infection. # NOT necessarily the ‘’second’’ dengue infection.
- 18. Old WHO classification WHO new classification
- 21. 2 – 7 days of illness + high grade fever Headache Retro – orbital pain Myalgia Arthralgia Rash & haemorrhagic manifestations positive tourniquet test petechiae
- 23. Signs & symptoms +
- 24. Criteria High fever/ recent history of acute fever A (+)ve tourniquet test Thrombocytopaenia <100,000 cells/mm3 Objective evidence of leaky capilaries •≥20% Elevated haematocrit •Pleural or other effusion - eg, ascites. •Low protein.
- 25. Dengue haemorrhagic fever is a dynamic disease 1. Febrile phase 2. Critical phase 3. Convalescent phase
- 27. When to suspect DF/DHF
- 30. Management as out patients Oral fluid (maintainance) Eg:-oral rehydration fluid, king coconut juice, fruit juices….etc Except plain water and red and brown drinks Rest & tepid sponging
- 31. Paracetamol 10-15mg/kg/dose (max 60mg/kg/day) Anti-emetics and H2 RB. NO NSAIDs or any STEROID Review with FBC , 1st after 3 days of onset Advice to return immediately for review…… if……
- 32. When to admit the patient ? Clinical judgment All patients with plt 100,000/mm3 All patients with warning signs
- 33. Following patients with probable dx of DF should admit. Infants Obese Major co-morbidities Adverse social circumstances
- 36. In DF & DHF ; lasts for 2-7 days Total WBC count initially high or normal drops < 5000/mm3
- 37. Platelet count Initially normal drops < 100,000/mm3 in 50% DF & 100% DHF Tender hepatomegaly DHF > DF Erythematous/ maculo-papular rash DHF < DF
- 38. Adequate fluid intake Total fluid requirement degree of dehydration (oral + IV) Maintenance volume Infants <6 months – 5% dextrose in N/2 Others – normal saline
- 39. Adequate physical rest Paracetamol 10-15mg/kg/dose (max 60mg/kg/day) NO all NAIDSs & STEROIDS Monitoring - ( Annexure iii) in the dengue guideline
- 41. Seen only in DHF late febrile phase; 3rd day to 7th day of illness up. Rapid drop in temperature Lasts for 24 – 48 hours DHF is a very dynamic disease.
- 42. Identifying the beginning & the end of the critical phase is a KEY FACTOR in guiding fluid therapy in DHF.
- 43. Leak starts slowly, increases gradually, peak around 24 hours, slows down and ceases around 48 hours. 0 5 10 15 20 25 30 0 20 40 60 .
- 44. Until the very last stage of shock; patient can appear conscious & very alert If Pulse Rate & Blood pressure NOT measured, early shock could be missed.
- 45. Platelets <100,000/mm3 Be Alert Patient may be in either of the, DF(50% of patients) DHF febrile phase DHF critical phase (early or late)
- 46. 1. 20% rise in the haematocrit
- 47. 2. Objective evidence detected radiologically Pleural effusion USS chest Chest X-ray Right Lateral decubitus Ascites : USS abdomen
- 48. 3. Biochemical parameters Serum albumin < 3.5g/dl or dropped by 0.5g/dl Serum cholesterol <100mg/dl or dropped by 20mg/dl ( NON fasting )
- 53. Calculation of the fluid quota (oral+IV) Max fluid intake during ENTIRE critical phase [Irrespective of its length] Maintenance + 5% deficit
- 54. Maintenance = 100ml/kg for 1st 10kg + 50ml/kg for next 10kg + 20ml/kg for the balance weight 5% deficit = 50ml/kg x body weight (kg)
- 55. Ideal body weight Weight for height [ BEST ] Weight for age BUT Actual body weight is taken for the calculations, if the actual weight < ideal weight Growth chart – 50th centile
- 56. Maximum weight = 50kg Maximum fluid intake = 4600ml
- 57. IV fluids N/2 +5% dextrose < 6 months infants N saline + 5% dextrose > 6 months; who is not taking orally for prolonged [ 50ml of 50% dextrose + 450ml N saline ]
- 58. A patient without shock IV normal saline/ Hartmann’s solution – largest possible size for the age. + oral fluids
- 59. Initially; oral +IV = 1.5ml/kg/hr Who can drink well = 0.5ml/kg/hr Pulse, BP, Pulse pressure, CRFT,HCT & UOP
- 60. UOP calculation Hourly UOP ; Best guide for the rate of infusion 0.5-1.0ml/kg/hr sufficient IF UOP >1.0 – too high infusion rates UOP <0.5 – inadequate fluids
- 62. A patient with shock Symptoms • Sweating • Abdominal pain • Restlessness • Altered conscious level
- 63. Signs • Cold extremities • CRFT > 2 sec • Unexplained tachycardia • Increased DBP • Narrowing pulse pressure 20mm/Hg
- 65. Mx of shock (if pulse & BP not picked up.) After 2 crystalloid boluses; Already having a fluid overload The full fluid quota given.
- 66. ONLY during the critical phase ONLY used as a bolus; Maximum over 1 hour. (10ml/kg/hr)
- 67. Dextran 40 – up to 3 doses within 24 hrs (10ml/kg/hr) 6% Starch – up to 5 doses within 24 hrs (10ml/kg/hr)
- 68. Stable vital signs HCT becomes normal Clinically improvement Diuresis
- 69. Lasts for 2-5 days Reabsorption of the extravasated fluid. Complications Fluid overload Hypocalaemia Nosocomial infections
- 73. No fever 24hrs, without antipyretics At least 2 days after recovery from shock Generally good & Increasing apetite Normal HCT for age.. [baseline around 38-40% when not known]
- 74. No distress from pleural effusion or ascitis Rising platelet count & >50,000/mm3 No other complication
- 76. Prolonged shock >4 hrs organ failure Liver failure 50% prognosis Liver + Renal 10% prognosis 3 organs(+ respiratory) very bad
- 77. Fluid overload Features :- Early- puffy eye lids, distended abdomen (ascites), tachypnoea, mild dyspnoea Late – Respiratory distress, SOB, & wheezing
- 78. A – acidosis B – Bleeding C – Calcium (hypocalcaemia) S – Sugar (hypoglycaemia)
- 79. Acidosis More prone to DIC & massive bleeding. pH < 7.35 (Arterial normal 7.35-7.45) HCO3- < 15 mmol/l (Arterial normal 22-24) Emperically NaHCO3 1ml/kg slow bolus (max 50ml) Diluted in equal volume of Normal Saline
- 80. Bleeding Ix for blood transfusion Overt bleeding Concealed bleeding ( HCT drop/metabolic acidosis)
- 81. Use Packed Red Cells 5ml/kg once 5ml/kg of PRC HCT by 5 points (eg:- 30 to 35) If HCT > 45%, blood given only after reducing HCT by a colloid.
- 82. Hypocalcaemia Mostly with ‘’convulsions’’ Measure serum Ca2+ levels Give calcium if complicated 1ml/kg of 10% Ca Gluconate,(max 10ml) Slow IV bolus over 15-20 mins Diluted in equal volume of NS Repeat 6 hourly
- 83. Hypoglycaemia Prevented by NS with 5% Dextrose •Dextrose saline (0.9% NaCl with 5% Dextrose) •Add 50ml 50% Dextrose to 450ml of 0.9% NaCl
- 84. Immediate goal plasma glucose at least 70mg/dl 10% dextrose, 2ml/kg by IV push Continue IV dextrose rate at 8mg/kg/min
- 85. Hyponatraemia Mainly due to Hyponatraemic fluids N/2 NaCl, N/5 NaCl, Water 3% NaCl is 3-5ml/kg Slow IV Through a larger vein; mostly a central vein
- 86. Encephalopathy Mainly - Hepatic encephalopathy Maintain cerebral perfusion pressure(CPP) Maintain - Mean arterial pressure (MAP) Reduce – Intra Cranial pressure (ICP) CPP = MAP - ICP
- 87. Airway oxygenation with O2 therapy Fluid management Maintain MAP Reduce ICP Maintain blood sugar level >70 mg/dl Maintain K+ & Na+ levels normal 3% NaCl if Na+ < 120meq/l
- 88. Vit K IV 3mg <1yr 5mg 1-5yrs, 10mg >5yrs IV Phenobarbitone - cerebral metabolism Controls seizures Gut cleaning NG tube Antibiotics – Metranidazole Lactulose
- 89. Platelet transfusion Recombinant factor vii Inotrops Steroids & IV immunoglobulins Fresh frozen plasma (FFP) Frusemide
- 90. Consider each patient as a dengue patient, as its presentation is changed. Avoid all NSAIDs & steroids. Correct diagnosis during early febrile phase improves the prognosis.
- 91. Identifying the beginning & the end of the critical phase is a key factor in guiding fluid therapy in DHF. Correct fluid management during the critical phase is the most important. Pulse pressure, HR, HCT & UOP Be concern about the possible complications.
- 95. THANK YOU