Oncologic Pathology Case Review
•
1 like•949 views

Oncologic Pathology_A Case-based Organ Systems Review

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Oncologic Pathology Case Review
Similar to Oncologic Pathology Case Review (20)
More from Imhotep Virtual Medical School
More from Imhotep Virtual Medical School (20)
Recently uploaded
Recently uploaded (20)
Oncologic Pathology Case Review
- 1. Oncologic Pathology A Case-based Organ Systems Review By: Marc Imhotep Cray MD
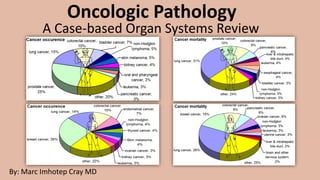
- 2. Marc Imhotep Cray, M.D. Cancer Incidence and Leading Causes of Cancer Death in Men and Women in U.S. 2 Cancers w highest incidence in men: Prostate cancer Lung cancer Colorectal cancer Leading causes of cancer deaths in men: Lung cancer Prostate cancer Colorectal cancer Cancers w highest incidence in women: Breast cancer Lung cancer Colorectal cancer Leading causes of cancer deaths in women: Lung cancer Breast cancer Colorectal cancer Learn more: Cancer Facts and Figures, 2020_American Cancer Society.pdf Important Note: Incidence of lung cancer and colorectal cancer both exceed incidence of prostate and breast cancer when data for men and women are combined.
- 3. Marc Imhotep Cray, M.D. Ten cancers commonly encountered on Boards: A Case-based Review (Hypertext opens to Video Edu.) 3 1. Gastric Cancer 2. Breast Cancer 3. Pancreatic Cancer 4. Lung Cancer 5. Prostate Cancer 6. Cervical Cancer 7. Brain Cancers 8. Thyroid Cancer 9. Colorectal Cancer 10.Endometrial Cancer
- 4. Marc Imhotep Cray, M.D. Vignette#1 4 A 54-year-old Japanese American man presents to the clinic complaining of a gnawing epigastric pain. Upon taking a complete history, you learn that he has lost 20 pounds over the last 2 months and has been vomiting after meals. The pain has not been relieved by the use of over the-counter antacids. On physical examination, you note supraclavicular lymph node swelling and darkened, thickened skin in the flexural areas of the patient’s legs and arms. You schedule the patient for an upper endoscopy with cytologic brushings and biopsies of any suspicious lesions as you fear that this patient may have a very serious condition. What is the Diagnosis?
- 5. Marc Imhotep Cray, M.D. Gastric Carcinoma 5 Etiology and Epidemiology: Risk factors include chronic gastritis, dietary nitrosamines, and excessive sodium intake; More common in men > 50 years of age and in patients with blood group A Pathology: Intestinal type: Gross: lesion with irregular necrotic base and heaped-up margins, usually located in lesser curvature of antrum or prepyloric region Microscopic: glandular formation of mucin-producing cells Diffuse type: Gross: infiltrative process producing rigid stomach wall (linitis plastica or leather bottle stomach); Microscopic: clusters of gastric-type mucous cells (signet-ring cells) within gastric wall; Can see early, aggressive, local metastasis to the lymph nodes and liver Clinical Manifestations: Presents with anorexia, weight loss, vomiting, and gnawing epigastric pain not relieved by antacids; Lab findings: Hypochromic microcytic anemia
- 6. Marc Imhotep Cray, M.D. Gastric Carcinoma cont. 6 Treatment: Surgical resection Note: Virchow node is involvement of left supraclavicular node by metastasis of stomach or other GI cancer Krukenberg tumor is bilateral metastasis of GI (usually stomach) cancer to ovaries • Histologically, tumor has abundant mucus and signet-ring cells Acanthosis nigricans refers to hyperpigmentation and epidermal thickening of flexural areas • It is suggestive of a visceral malignancy, including cancer of stomach, lung, breast, or uterus
- 7. 7 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 8. 8 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 9. 9 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 10. 10 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 11. 11 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 12. Marc Imhotep Cray, M.D. Gastric Adenocarcinoma: Key Points 12 Presentation of gastric adenocarcinoma is very similar to that of peptic ulcer disease and gastroesophageal reflux disease From 60% to 90% of cases of distal gastric adenocarcinoma are attributed to chronic Helicobacter pylori infection An ulcerated gastric lesion should always be biopsied b/c as many as 5% may harbor gastric cancer cells Adenocarcinoma comprises almost all gastric cancers and can be classified by gross or microscopic pathologic appearance Adenocarcinoma may produce distinct lesions or may infiltrate the stomach diffusely
- 13. Marc Imhotep Cray, M.D. Vignette #2 13 A 50-year-old woman presents to your clinic after finding a mass on the upper outer quadrant of her left breast. After taking a thorough history, you learn that her mother died from breast cancer and her maternal aunt was also diagnosed with breast cancer at an early age. The patient started her period at age 11, did not bear any children, and has not been through menopause. On physical examination, she is markedly obese and you notice retraction of the skin and the nipple on her left breast. You locate the mass in question during your breast examination and find that it is fixed, hard, and nontender. The mass was not present on her last mammogram dating back 2 years. You also feel palpable axillary lymph nodes. You schedule the patient for an immediate mammography and needle biopsy to confirm your suspicions. What is the Diagnosis?
- 14. Marc Imhotep Cray, M.D. Breast Carcinoma 14 Etiology and Epidemiology: Risk factors include: Family history of first-degree relative with breast cancer at young age (highest risk), Autosomal dominant inheritance of mutations in BRCA1 or BRCA2 gene, female gender, Increased age, Early first menarche, Delayed first pregnancy, Nulliparity, Late menopause, Radiation exposure, and exogenous estrogen use
- 15. Marc Imhotep Cray, M.D. Breast Cancer Morphology 15 Most common location of tumors within breast is in upper outer quadrant (50%), followed by central portion (20%) About 4% of women with breast cancer have bilateral primary tumors or sequential lesions in the same breast Breast cancers are classified morphologically according to whether they have penetrated the basement membrane • Those that remain within this boundary are termed in situ carcinomas, and • those that have spread beyond it are designated invasive carcinomas
- 16. Marc Imhotep Cray, M.D. Breast Cancer Morphology cont. 16 In classification, above main forms of breast carcinoma are as follows: A. Noninvasive 1. Ductal carcinoma in situ (DCIS) 2. Lobular carcinoma in situ (LCIS) B. Invasive 1. Invasive ductal carcinoma (includes all carcinomas that are not of a special type)-70% to 80% 2. Invasive lobular carcinoma- 10% to 15% 3. Carcinoma with medullary features-5% 4. Mucinous carcinoma (colloid carcinoma) -5% 5. Tubular carcinoma-5% 6. Other types Adapted from: Kumar, V; Abbas AK (Eds.), Robbins Basic Pathology, 10th Ed. Philadelphia, Pa : Elsevier, 2018;742.
- 17. 17 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 18. 18 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 19. 19 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 20. Marc Imhotep Cray, M.D. Breast Cancer: Key Points 20 Nontender, firm breast masses with poorly delineated margins are concerning for invasive breast cancer Other findings concerning for breast cancer include nipple discharge, nipple scaling, breast asymmetry, nipple inversion, peau d’orange, erythema, and warmth. Most common cause of breast masses in young women is fibroadenoma BRCA1 and BRCA2 mutations predispose to development of breast cancer and account for approximately 25% of familial breast cancer syndromes
- 21. Marc Imhotep Cray, M.D. Breast Cancer: Key Points (2) 21 BRCA1 mutations additionally confer increased risk for development of ovarian cancer Most breast cancers arise from the intermediate ducts and are invasive (invasive ductal carcinoma) Ductal carcinoma in situ (DCIS) is thought to progress to invasive ductal carcinoma in most women Lobular carcinoma in situ (LCIS) progresses to invasive lobular carcinoma in some women but not at the same rate of DCIS progression Estrogen receptor/progesterone receptor (ER/PR) and HER2/neu (ERBB2) are important biomarkers and may guide adjuvant therapy for breast cancer following resection
- 22. Marc Imhotep Cray, M.D. Vignette #3 22 A 78-year-old man presents with a 2-month history of epigastric pain. He describes the pain as a vague pressure that occasionally radiates to his back. It does not reliably occur before or after meals. He has lost 20 lb in the last 2 months, though he attributes this to his recent lack of appetite. He has taken NSAIDs with no relief. The pain occasionally subsides when he leans forward while sitting up. He smoked two packs of cigarettes per day for 35 years but quit 2 years ago. Examination is significant for scleral icterus and a nontender palpable gallbladder. What is the Diagnosis?
- 23. Marc Imhotep Cray, M.D. Pancreatic carcinoma 23 Pancreatic carcinoma is likely Pain is present in over 70% of cases of pancreatic carcinoma and often radiates to the back Weight loss is suggestive of underlying neoplasm but may also be related to depressive symptoms often seen in pancreatic cancer Scleral icterus indicates obstruction of biliary ductal system Courvoisier’s sign describes the finding of a nontender palpable gallbladder on abdominal examination and also indicates obstruction of the biliary ductal system Courvoisier’s sign is more commonly seen in obstruction by a neoplasm, whereas scleral icterus results from obstruction by any mechanism Pancreatic carcinoma - causes, symptoms, diagnosis, treatment, pathology_Osmosis
- 24. Marc Imhotep Cray, M.D. Pancreatic Ca Risk Factors 24 Acquired risk factors include cigarette smoking (note that this patient was a smoker), industrial chemical exposure, type 2 diabetes mellitus, and obesity Hereditary risk factors include a family history of pancreatic cancer (7-8% of pancreatic cancer patients have a first-degree relative with pancreatic cancer, versus 0.6% of control subjects) and a familial form of chronic pancreatitis • The following familial cancer syndromes also confer an increased risk of developing pancreatic cancer: o Peutz-Jeghers syndrome o Ataxia-telangiectasia o Hereditary nonpolyposis colorectal cancer (HNPCC) o Familial breast cancer (BRCA2-positive)
- 25. 25 Pancreatic Ca Tumor Location Impacts Symptoms Location of tumor in pancreas affects types of symptoms and how soon they might start to show For example, jaundice symptoms may appear when tumor obstructs the head of pancreas If tumor is in body or tail of pancreas, pain and weight loss might be more likely • Pancreatic cancer in body or tail can also take longer to present w Sx, allowing tumor more time to grow or metastasize before it’s found https://www.hopkinsmedicine.org/health/conditions-and- diseases/pancreatic-cancer/pancreatic-cancer-symptoms Where would a pancreatic mass most likely be located in order to cause biliary obstruction? Ans. Pancreatic head Two thirds of pancreatic cancers are located in head of pancreas, where they can easily obstruct the biliary ductal system One third of pancreatic cancers occur in the body or tail
- 26. Marc Imhotep Cray, M.D. Pancreatic Cancer Gene Mutations 26 The KRAS gene is activated by a point mutation in 80% to 90% of pancreatic cancers cause a deactivation of protein product’s guanosine triphosphatase activity as a result, protein is constitutively active Ras activates multiple other intracellular signaling pathways The p16 gene (important in cell cycle control) is most frequently inactivated tumor suppressor gene inactivated in 95% of pancreatic cancers Many other mutations also occur in pancreatic cancers For example, all pancreatic cancers and 83% of colon cancers have at least one mutational event in a TGF-β pathway
- 27. Marc Imhotep Cray, M.D. Histologic types of pancreatic cancer 27 Pancreatic adenocarcinoma: >90%Neoplastic cells arise from ductal cells of pancreas form ductules and may even secrete mucin Neuroendocrine tumors: <5% Arising from neuroendocrine cells of pancreas tend to be less invasive and have a better prognosis Cystic tumors: <5% These tumors may be benign or malignant also less aggressive than adenocarcinoma
- 28. Marc Imhotep Cray, M.D. Pancreatic Adenocarcinoma Tx & Px 28 Px is poor Tumors located in body or tail have an even poorer prognosis than those located in head b/c they often do not produce Sn & Sx until they have invaded adjacent structures Tx: Surgical resection offers a median survival time of 18 months and a 5 year survival rate of approx. 5-20% • When tumors are not resectable, median survival time is 4 to 8 months • Only 10% to 15% of all tumors are resectable at presentation
- 29. Marc Imhotep Cray, M.D. Vignette #3 cont’ed. 29 An abdominal computed tomography (CT) scan reveals a mass at the head of the pancreas. The splenic vein is completely occluded by clot, and there is invasion of the superior mesenteric artery. No metastases are seen. The tumor is deemed unresectable, and he is offered palliative care. What serum cancer marker is likely to be elevated in this patient? Ans. CA 19-9 However, CA 19-9 lacks sufficient sensitivity (50-75%) and specificity (approx. 85%) to be used in the screening of asymptomatic individuals However, CA 19-9 may be followed postoperatively in order to assess disease progression or regression
- 30. Marc Imhotep Cray, M.D. Vignette #3 cont’ed. 30 The patient returns to the office 1 month later and is noted to have a random glucose of 180 mg/dL. He also complains of pain in his right calf. On examination of his leg, you note a superficial palpable cord that is tender. A fasting glucose drawn 2 days later is 124 mg/dL. What two processes have developed in this patient? Glucose intolerance tends to develop after Dx of pancreatic Ca has been made due to destruction of normal pancreatic beta cells and ducts by tumor Peripheral venous thrombosis (superficial thrombophlebitis) has developed Patients w cancer are at an increased risk for clotting and frequently develop both deep and peripheral venous thromboses When migratory peripheral venous thromboses are noted in a pt. w pancreatic cancer, it is called Trousseau’s syndrome or Trousseau’s sign NB: DVT and PE are most common thrombotic conditions in pts w cancer
- 31. 31 Adenocarcinoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 32. 32 Adenocarcinoma, CT image Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 33. 33 Adenocarcinoma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 34. Marc Imhotep Cray, M.D. Pancreatic Cancer: Key Points 34 Pain is frequently present in pts. w pancreatic adenocarcinoma & may radiate to back • Painless jaundice is another important presentation for pancreatic adenocarcinoma Courvoisier’s sign refers to a nontender distended gallbladder palpable on examination CA 19-9 levels are typically elevated in pancreatic adenocarcinoma • Although not helpful for screening asymptomatic patients, they may be helpful in diagnosing a patient suspected of having pancreatic cancer • May also be helpful in following disease progression KRAS and p16 are two common genetic mutations found in pancreatic adenocarcinoma Glucose intolerance and Trousseau’s syndrome are among the many complications of pancreatic cancer
- 35. Marc Imhotep Cray, M.D. Vignette #4_Part 1 35 A 63-year-old man presents to your office after noticing that his left eyelid is droopy. Upon further questioning, he admits to some shortness of breath over the past 2 months, but attributes that to his 40-year-long heavy smoking habit. Physical examination reveals ptosis and miosis of the left eye and extremely dry skin of the left face. A chest x-ray demonstrates an irregular mass in the apex of his left lung. You admit the patient to the hospital for a biopsy of the mass, but you fear that the prognosis is not good. What is the Diagnosis?
- 36. Marc Imhotep Cray, M.D. Bronchogenic Carcinoma 36 Etiology: Cigarette smoking (especially linked w squamous cell and small cell carcinoma); air pollution; ionizing radiation; asbestos; nickel; chromium exposure Pathology: Squamous cell: Central location; hilar mass with cavitation; keratinization of squamous cells Adenocarcinoma: Peripheral location; includes two forms: (1) Bronchial derived: develops on scar site, glandular elements w mucin cells; (2) Bronchioloalveolar: multiple mucinous nodules (which appear on CXR), tall columnar epithelial cells, which line the alveolar walls Small cell: Central location; small, round, basophilic cells with little cytoplasm (oat cell is a neoplasm of neuroendocrine Kulchitsky cells) Large cell: Peripheral location; large polygonal undifferentiated cells (pleomorphic giant cells w leukocyte fragments in cytoplasm)
- 37. Marc Imhotep Cray, M.D. Bronchogenic Ca cont’ed. 37 Pathology cont’ed. Metastases of all types often occur to adrenals, brain, liver, bone Important Notes: Metastases of other cancers to lung are more common than primary lung cancer and may spread to lung hematogenously, via lymphatics or through contiguous growth Carcinoid tumor can also occur in the lung
- 38. Marc Imhotep Cray, M.D. Vignette #4_Part 2 38 A 71-year-old man presents to your office because of water retention. He states that he keeps himself well-hydrated, but he does not feel that his intake matches his output. Pertinent past medical history includes shortness of breath and weight loss of 15 pounds over the past 3 months. He has smoked 2 1/2 packs of cigarettes per day for 50 years. Besides looking into possible causes of urinary obstruction and other diagnoses, you decide to send the man for a chest x-ray, which reveals a central coin lesion. Based on the patient’s history, you expect to see small, round cells with scant cytoplasm on a biopsy of the mass. What s the Diagnosis?
- 39. Marc Imhotep Cray, M.D. Bronchogenic Ca cont’ed 39 Clinical Manifestations: Hemoptysis; chest pain; dyspnea; cough; weight loss; pleural effusion (usually bloody); hoarseness (from recurrent laryngeal nerve paralysis) Pancoast tumor: apical lung tumor resulting in Horner syndrome (ptosis, miosis, anhidrosis) owing to tumor involvement of cervical sympathetic plexus Superior vena cava syndrome: facial swelling and dilation of veins of head and upper limbs from tumor compression of SVC Cushing syndrome (caused by ACTH-like protein production), SIADH (caused by ADH-like protein production), and Lambert-Eaton syndrome (myasthenia gravis-like illness resulting from defect in acetylcholine release) are all seen in small cell carcinoma • Imaging: CXR demonstrates pneumonic coin lesion • Lab findings: Hypercalcemia (caused by PTH-like protein production) seen in squamous cell carcinoma
- 40. Marc Imhotep Cray, M.D. Bronchogenic Ca cont’ed 40 Treatment and Prognosis: Surgery, radiation, and chemotherapy for nonsmall cell lung carcinoma; radiation and chemotherapy for small cell carcinoma Overall 5-year survival rate is 10%–15%
- 41. Bronchogenic carcinoma, gross The large carcinoma ( ) in the upper lobe is arising in a lung with centriacinar emphysema, suggesting cigarette smoking as the risk factor There are patchy infiltrates in lower lobe representing pneumonia, likely from central airway obstruction by this large mass There is inferior congestion, likely exacerbated by heart failure Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 42. 42
- 43. 43 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 44. 44 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 45. Marc Imhotep Cray, M.D. Lung Cancer: Key Points 45 Acute bronchitis is the most common cause of hemoptysis • However, hemoptysis is also concerning for lung cancer and tuberculosis Most common presentations of lung cancer are: • Asymptomatic pulmonary nodule • Change in “smoker’s cough” • Nonpurulent “pneumonia” in an adult • Persistent upper respiratory infection • Hemoptysis • Hoarseness • Sn & Sx of metastatic disease • Sn & Sx of paraneoplastic syndrome
- 46. Marc Imhotep Cray, M.D. Lung Cancer: Key Points cont’ed. 46 Approximately 90% of lung cancers occur in smokers Four most common histologic types of primary lung cancer are squamous cell carcinoma, adenocarcinoma, large cell carcinoma, and small cell carcinoma Small cell lung cancer (SCLC) and non–small cell lung cancer (NSCLC) behave very differently and have markedly different prognoses Lung cancer can produce symptoms by local tumor growth, regional spread, or metastatic disease
- 47. Marc Imhotep Cray, M.D. Vignette #6 47 An 81-year-old man presents to the clinic complaining of pain with urination. On taking a complete history, you learn that he has had difficulty in starting and stopping the stream of urine for the last 4 months and has recently been suffering from severe back pain. On physical examination, you perform a digital rectal examination and find a large palpable prostate nodule, which is firm and irregularly shaped. You fear that laboratory tests will demonstrate an increased total PSA with a decreased fraction of free PSA and may also demonstrate an increase in serum alkaline phosphatase. You immediately refer the patient to a urologist for prostatic biopsy. What is the Diagnosis?
- 48. Marc Imhotep Cray, M.D. Prostate Carcinoma 48 Epidemiology: Most common cancer among men and second leading cause of cancer death in men; Occurs in men > 50 years of age Pathology: Gross: Irregular nodules arising from peripheral group of glands (peripheral zone of posterior lobe is most common) Microscopic: Adenocarcinoma with well-defined glands lined by cuboidal cells with large nuclei and prominent, large nucleoli; • May also be undifferentiated with cells growing in cords or sheets • Often see invasion of vascular or lymphatic vessels of prostatic capsule • In later stages, may progress to bony osteoblastic metastasis via hematogenous spread NB: The most common acquired mutations in prostatic carcinomas create TPRSS2-ETS fusion genes or act to enhance P13K/AKT signaling, which promotes tumor cell growth and survival
- 49. Marc Imhotep Cray, M.D. Prostate Ca cont. 49 Clinical Manifestations: Frequently asymptomatic, but may present with dysuria, increased urinary frequency or back pain (if metastasis to bone); most often diagnosed on digital rectal examination with palpation of irregular, enlarged, firm nodule with confirmation of diagnosis via prostatic biopsy Lab findings: Increased serum PSA and prostatic acid phosphatase (useful tumor markers for disease progression), Increased total PSA with decreased fraction of free PSA (Contrastly, BPH has Increased total PSA w proportionate increase in fraction of free PSA) Increased serum alkaline phosphatase (if osteoblastic metastasis)
- 50. 50 Prostate Ca cont. Treatment and Prognosis: Prostatectomy; radiotherapy; GnRH analogues (leuprolide); antiandrogens (eg, flutamide); chemotherapy Can have an indolent or aggressive course as predicted by Gleason system of grading, which is based on differentiation of tumor NB: PSA testing and digital rectal examination should be offered annually for screening purposes beginning at age 50
- 51. 51 Prostatic intraepithelial neoplasia and adenocarcinoma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 52. 52 Adenocarcinoma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 53. 53 (A) Adenocarcinoma of the prostate demonstrating small glands crowded in between larger benign glands. (B) Higher magnification shows several small malignant glands with enlarged nuclei, prominent nucleoli, and dark cytoplasm, as compared with the larger, benign gland (top). Kumar V and Abbas AK. Robbins and Cotran Basis Pathology, 10th Ed. Philadelphia: Saunders, 2018, Fig 18-14, Pg. 701.
- 54. 54 Adenocarcinoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 55. Marc Imhotep Cray, M.D. Adenocarcinoma of the prostate. Carcinomatous tissue is seen on posterior aspect (lower left). Note the solid whiter tissue of cancer, in contrast with spongy appearance of benign peripheral zone on contralateral side. 55 Kumar V and Abbas AK. Robbins and Cotran Basis Pathology, 10th Ed. Philadelphia: Saunders, 2018, Fig 18-13, Pg. 700.
- 56. 56 Adenocarcinoma, gross (3) Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 57. 57 Prostatic cancer: Key Points 70% of prostatic tissue is in the peripheral zone 70% of prostate cancer cases arise in the peripheral zone Peripheral zone is the only area accessible via digital rectal examination Most cases of prostate cancer are asymptomatic and detected by abnormal findings on digital rectal examination or elevated prostate-specific antigen (PSA) PSA can be elevated in prostate cancer, benign prostatic hyperplasia (BPH), or prostatitis Only a small number of men who develop prostate cancer will die as a result of it Screening with annual PSA levels may allow detection of prostate cancer at earlier stages Prognosis of prostate cancer is determined by Gleason grade (2-10) and tumor staging (TNM system) Prostate cancer spreads by local extension and metastases to bone (especially axial skeleton) and pelvic lymph nodes
- 58. Marc Imhotep Cray, M.D. Vignette #5 58 A 42-year-old woman presents to the clinic complaining of postcoital bleeding and vaginal discharge. She complains of a 3-month history of spotting in her underwear after intercourse and an odorous vaginal discharge that is not purulent. Her social history is significant for past practice of prostitution and her past medical history is significant for several STDs that were appropriately treated. She has not had a routine PAP smear in over 10 years. After a PAP smear reveals abnormal cells, you perform a cervical biopsy, worrying that you may find invasive malignant cells in the cervix and adjacent koilocytosis. You fear that the patient will need to undergo a hysterectomy with possible adjunct radiation therapy if your suspected diagnosis is confirmed. What is the Diagnosis?
- 59. Marc Imhotep Cray, M.D. Dysplasia, Carcinoma in Situ, and Squamous Cell Carcinoma of the Cervix 59 Etiology and Epidemiology: Associated with human papilloma virus (HPV) types 16, 18, 31, and 33, early age of first intercourse and multiple sexual partners Occurs most commonly between the ages of 30 and 45 Pathology: Cervical dysplasia: Involves squamocolumnar junction; characterized by cells with hyperchromatic nuclei, irregular nuclear contours, and scant cytoplasm; epithelial growth begins at basal layer extending outward; classified as Cervical Intraepithelial Neoplasia (CIN) Subtypes Grades I-III (or Squamous Intraepithelial Lesions Low-grade to High-grade ) CIN I (LSIL) is characterized by atypical undifferentiated cells only in lower third of epithelium, whereas CIN II (HSIL) superficial layer of cells still shows differentiation and koilocytosis CIN III (HSIL) has atypia through > 2/3 thickness of epithelium, koilocytotic change usually is absent
- 60. Marc Imhotep Cray, M.D. Dysplasia, Carcinoma in Situ, and Squamous Cell Carcinoma of the Cervix (2) 60 Pathology cont: Cervical carcinoma in situ (CIS): Dysplastic cells extending through entire epithelium, but without invasion of basement membrane Invasive cervical carcinoma (ICC): Gross: can be exophytic, ulcerating, or infiltrating mass Microscopic: usually squamous cell carcinoma with large cells and keratinization; can be adenocarcinoma or undifferentiated carcinoma; arises from preexisting CIN at squamocolumnar junction; non-neoplastic epithelial cells often demonstrate koilocytosis (assoc. w. HPV infection) Koilocytes, also known as halo cells, are a type of epithelial cell that develops following a human papillomavirus (HPV) infection; They are structurally different from other epithelial cells, in that, their nuclei are an irregular size, shape, or color
- 61. Marc Imhotep Cray, M.D. Natural History of Squamous Intraepithelial Lesions (SILs) 61 Lesion Regress Persist Progress LSIL (CIN I) 60% 30% 10% (to HSIL) HSIL (CINII,III) 30% 60% 10% (to carcinoma)* *Progression within 10 years. LSIL, Low-grade SIL; HSIL, high-grade SIL Redrawn after Kumar V and Abbas AK. Robbins and Cotran Basis Pathology, 10th Ed. Philadelphia: Saunders, 2018, Fig. 19.1 , Pg. 718. Remember: Cervical Intraepithelial Neoplasia (CIN) Subtypes Grades I-III (or Squamous Intraepithelial Lesions Low-grade to High-grade ) CIN I (LSIL) is characterized by atypical undifferentiated cells only in lower third of epithelium, whereas, CIN II (HSIL) superficial layer of cells still shows differentiation and koilocytosis CIN III (HSIL) has atypia through > 2/3 thickness of epithelium, koilocytotic change usually is absent
- 62. 62 Three Stages of squamous intraepithelial lesions (SIL) Spectrum of squamous intraepithelial lesions (SIL) with normal squamous epithelium for comparison: LSIL with koilocytotic atypia; HSIL w progressive atypia in all layers of the epithelium; and HSIL w diffuse atypia and loss of maturation (carcinoma in situ, far right image) Kumar V and Abbas AK. Robbins and Cotran Basis Pathology, 10th Ed. Philadelphia: Saunders, 2018, Fig. 19.6 , Pg. 719.
- 63. 63 Cytologic features of squamous intraepithelial lesion (SIL) in a Papanicolaou Smear Superficial squamous cells may stain either red or blue. (A) Normal exfoliated superficial squamous epithelial cells. (B) Low-grade squamous intraepithelial lesion (LSIL). (C and D) Both high-grade squamous intraepithelial lesions (HSILs). Note the reduction in cytoplasm and the increase in the nucleus-to-cytoplasm ratio as the grade of the lesion increases. This observation reflects progressive loss of cellular differentiation on surface of cervical lesions from which these cells are exfoliated Kumar V and Abbas AK. Robbins and Cotran Basis Pathology, 10th Ed. Philadelphia: Saunders, 2018, Fig. 19.7 , Pg. 719.
- 64. Marc Imhotep Cray, M.D. Dysplasia, Carcinoma in Situ, and Squamous Cell Carcinoma of Cervix (3) 64 Clinical Manifestations: ICC: Irregular vaginal bleeding; postcoital spotting; cervical ulceration; nonpurulent discharge; dysuria; invasive disease can obstruct ureters and lead to renal failure Treatment ICC: Hysterectomy; radiation therapy; prevention with HPV vaccine NB: Screening for cervical cancer with PAP smears should begin 3 years after intercourse and no later than age 21 and continue every 1–3 years until age 70
- 65. 65 Human papillomavirus effect, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 66. 66 Cervical squamous dysplasia, Pap smear Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 67. 67 Cervical squamous carcinoma, Pap smear Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 68. 68 Squamous cell carcinoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 69. 69 Squamous cell carcinoma, gross (2) Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 70. 70 Squamous cell carcinoma, gross (3) Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 71. 71 Cervical Cancer: Key Points Invasive cervical carcinoma typically manifests with abnormal vaginal bleeding or postcoital spotting Invasive cervical carcinoma most often occurs in the transformation zone of the cervix, between original squamocolumnar junction and new squamocolumnar junction Cervical carcinoma is a sexually transmitted disease, the etiologic agent of which is human papillomavirus (HPV) (most frequently types 16 and 18); therefore, risk factors are primarily related to sexual behaviors Squamous cell carcinoma is the most frequent histologic type, occurring in 75% of cases The Papanicolaou (Pap) smear has markedly reduced the incidence of invasive cervical cancer in America as a result of its ability to screen for preinvasive lesions
- 72. Marc Imhotep Cray, M.D. Vignette #6 72 A 59-year-old man presents to your office complaining of severe headaches for the last week. He tells you that his headaches are often associated with projectile vomiting. Physical examination reveals bilateral papilledema and a CT scan of the head demonstrates an irregular mass in the left cerebral hemisphere. When a CT-guided brain biopsy demonstrates pseudopalisading malignant cells around areas of necrosis, you realize that this patient’s prognosis is very poor. What is the Diagnosis?
- 73. Marc Imhotep Cray, M.D. Glioblastoma Multiforme 73 Etiology and Epidemiology: Assoc. w genetic mutations in several oncogenes and tumor-suppressor genes, including TP53 (p53), RB gene (Learn them, First AID 2020, Pg. 224.) Most common primary brain neoplasm Occurs most frequently betw. ages 40 and 60 Pathology (GBM is a Grade IV astrocytoma) Gross: Variable, noncircumscribed lesion found in cerebral hemisphere Microscopic: High-grade astrocytoma (arises from astrocytes); central areas of necrosis and hemorrhage surrounded by multiple tumor cells, arranged in a pseudopalisading fashion; high degree of anaplasia
- 74. Marc Imhotep Cray, M.D. Glioblastoma Multiforme (2) 74 Clinical Manifestations: Seizures; headaches; nausea and vomiting; other signs of increased intracranial pressure Imaging: Mass effect, cerebral edema Treatment and Prognosis: Surgical resection w chemotherapy and radiation Px is very poor w most pts. dying within a year of Dx Note: Low-grade astrocytomas, especially pilocytic astrocytomas, are benign, slow- growing tumors occurring in cerebellum of children On histology, Rosenthal fibers (eosinophilic, corkscrew fibers) are present
- 75. 75 Glioblastoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Saunders, 2015.
- 76. 76 Glioblastoma, MRI Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Saunders, 2015.
- 77. 77 Glioblastoma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Saunders, 2015.
- 78. Marc Imhotep Cray, M.D. Vignette #7 78 A 42-year-old woman presents to your office complaining of headaches and vomiting over the past 4 months. Upon further questioning, you learn that she also feels as if she trips more than usual when she is walking and she has recently had more trouble remembering things. A physical examination reveals bilateral papilledema and reduced strength and hyperreflexia in both of her legs. A CT scan reveals a parasagittal mass compressing the brain and a CT-guided brain biopsy demonstrates a whorled pattern of tumor cells with psammoma bodies. You tell the patient that she will most likely need surgery to remove the tumor. What is the Diagnosis?
- 79. Marc Imhotep Cray, M.D. Meningioma 79 Etiology and Epidemiology: Benign, slow-growing tumor arising from meningothelial cells of arachnoid; therefore external to brain Multiple meningiomas can be present in pts w neurofibromatosis type 2 Occurs most often in women after age 30 Pathology: Gross: Usually round encapsulated mass w dural base; usually occurs in convexities of cerebral hemispheres or parasagittal region; usually does not infiltrate brain Microscopic: Whorled pattern of tightly packed tumor cells; psammoma bodies (laminated calcifications)
- 80. Marc Imhotep Cray, M.D. Meningioma (2) 80 Clinical Manifestations: Sx are assoc. w compression of underlying brain including seizures, headaches, N/V and other signs of increased ICP Treatment and Prognosis: Surgical removal of tumor Prognosis is good Of Note: Meningiomas are second most common primary brain tumors
- 81. 81 Meningioma, MRI Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Saunders, 2015.
- 82. 82 Meningioma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Saunders, 2015.
- 83. 83 Meningioma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Saunders, 2015.
- 84. Marc Imhotep Cray, M.D. Vignette #8 84 A 49-year-old man presents to the emergency department with a seizure. When he has been stabilized, he tells you that he has had several severe headaches over the past couple of months. A CT scan of his head reveals a large mass in the frontal lobe of his brain that demonstrates areas of calcification. You admit him to the neurology service and you suspect that he will need surgery to treat his condition. What is the Diagnosis?
- 85. Marc Imhotep Cray, M.D. Oligodendroglioma 85 Etiology and Epidemiology: Relatively rare benign tumor derived from oligodendrocytes; Commonly affects middle-aged people Pathology: Gross: Circumscribed, slow-growing gray mass often w cysts; usually occurs in white matter of cerebral hemispheres (especially frontal lobe) Microscopic: Sheets of uniform cells with round nuclei with clear cytoplasm (fried egg appearance); often calcification is present; increased vascularity (“Chicken-wire” capillary pattern) Clinical Manifestations: Seizures; headaches; papilledema; other signs of increased intracranial pressure (ICP) Imaging: Calcification of tumor is detected on CT scan Treatment and Prognosis: Surgical resection, followed by radiotherapy and chemotherapy Average survival time is 5–10 years after diagnosis
- 86. 86 Oligodendroglioma, MRI and microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Saunders, 2015.
- 87. Marc Imhotep Cray, M.D. Vignette #9 87 A 58-year-old woman presents to your clinic complaining of hearing loss and a ringing in her left ear. The Weber and Rinne hearing tests help you to determine that the hearing loss is caused by a sensory disturbance and not a conduction deficit. You send the patient for an MRI of her head, which reveals a mass at the left cerebellopontine angle, impinging on cranial nerve VIII. You refer this patient to a neurosurgeon for a biopsy and likely removal of the mass. What is the Diagnosis?
- 88. Marc Imhotep Cray, M.D. Schwannoma (an acoustic neuroma) 88 Etiology: Usually benign tumors arising from Schwann cells Bilateral acoustic schwannomas are assoc. w neurofibromatosis type 2 Pathology: Gross: Encapsulated masses, often with cystic areas; usually occur in cerebellopontine angle where it can compress cranial nerve VIII (acoustic schwannoma) Microscopic: Two growth patterns: (1) Antoni A: tightly packed elongated cells with palisading nuclei (2) Antoni B: loose arrangement of cells w microcysts
- 89. Marc Imhotep Cray, M.D. Schwannoma (2) 89 Clinical Manifestations: Presents w Sx assoc. w compression of involved nerve (cranial nerve VIII compression leads to pts. presenting w ipsilateral hearing loss, tinnitus, and vertigo), seizures, headaches, N/V, and other signs of increased ICP Treatment and Prognosis: Surgical resection of tumor Prognosis is good Note: Pineal tumors usually occur in young men betw. ages of 10 and 40 Presents w Parinaud syndrome (paralysis of upward gaze caused by pre-tectal and superior colliculus damage, Obstructive hydrocephalus [owing to compression of aqueduct of Sylvius], and Endocrine abnormalities [owing to compression of hypothalamus])
- 90. 90 Schwannoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 91. 91 Schwannoma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 92. Marc Imhotep Cray, M.D. Vignette #10 92 A 6-year-old boy presents to his pediatrician’s office complaining of frequent falls. Upon further questioning, you learn that the boy has also been suffering from nausea and vomiting, which is usually associated with headaches. During physical examination, you note that the boy has an ataxic gait and bilateral papilledema. You send the boy for a CT scan, which reveals a mass in the cerebellum and dilated third and lateral ventricles. You immediately refer the patient to a neurosurgeon. What is the Diagnosis?
- 93. Marc Imhotep Cray, M.D. Medulloblastoma 93 Etiology and Epidemiology: Highly malignant tumor arising in cerebellum; assoc. w deletion on short arm of chr 17 (17p-) Occurs mostly in children and accounts for 20% of all brain tumors in children Pathology Gross: Gray, well-circumscribed tumor located at midline of cerebellum Microscopic: Hypercellular sheets of anaplastic cells, demonstrating many mitoses, scant cytoplasm, and hyperchromatic nuclei; cells are often arranged in a rosette or perivascular pseudorosette formation (called Homer Wright rosettes)
- 94. Marc Imhotep Cray, M.D. Medulloblastoma (2) 94 Clinical Manifestations: Unsteady gait; obstructive hydrocephalus (tumor may obstruct flow of CSF by compressing fourth ventricle); seizures, headaches; N/V; other signs of increased ICP Treatment and Prognosis: Surgery w radiation and ChemoTx With total excision and radiation, 5-year survival rate is 75%
- 95. 95 Medulloblastoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 96. 96 Medulloblastoma, MRI Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 97. 97 Medulloblastoma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 98. Marc Imhotep Cray, M.D. Vignette #11 98 An 8-year-old girl presents to your clinic complaining of blurry vision. During physical examination, you note bilateral papilledema. A CT scan of the head demonstrates a mass extending from the floor of the fourth ventricle and dilated lateral and third ventricles. You suspect that a biopsy of the mass would demonstrate cells with blepharoplasts in a perivascular pseudorosette arrangement. What is the Diagnosis?
- 99. Marc Imhotep Cray, M.D. Ependymoma 99 Etiology and Epidemiology: Tumor arising from ependyma of ventricular system Most commonly occur in children (usually in fourth ventricle), but can occur in spinal cord of adults Pathology: Gross: Solid, papillary masses extending from floor of fourth ventricle Microscopic: Uniform cells w round nuclei set in a fibrillary stroma and arranged in a perivascular pseudorosette formation; tumor cells often have blepharoplasts (rod near nucleus, which represents basal ciliary bodies)
- 100. Marc Imhotep Cray, M.D. Ependymoma (2) 100 Clinical Manifestations: Obstructive hydrocephalus (tumor may obstruct flow of CSF through compression of fourth ventricle); seizures; headaches; N/V; other signs of increased ICP Treatment and Prognosis: Surgical excision (difficult owing to proximity of brainstem nuclei) Px is poor w average survival time of 4 years
- 101. 101 Ependymoma, CT image Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 102. 102 Ependymoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 103. 103 Ependymoma, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 104. Marc Imhotep Cray, M.D. Brain Cancers: Key Points 104 Meningiomas are the most common type of primary brain tumor, occurring in 27% of cases Astrocytomas arise from astrocytes and are divided into four grades based on histologic appearance. Of these grades, glioblastoma multiforme has the worst prognosis Glioblastoma multiforme is distinctive because of endothelial proliferation and necrosis • “Pseudopalisading” is often seen in glioblastoma multiforme Uncal herniation syndrome results from hippocampal gyrus herniation through the tentorial notch • Herniation produces pressure on the posterior cerebral artery and brain stem Herniation is caused by an increase in pressure in one intracranial compartment • This pressure increase is due not only to the presence of a space-occupying lesion but also to significant edema in the parenchyma surrounding the lesion
- 105. Marc Imhotep Cray, M.D. Thyroid Cancer 105 Malignant thyroid tumors cause 0.4% of all cancer deaths in US Approximately 10,000 new cases are diagnosed each year Mortality from thyroid cancer exceeds that from malignant tumors of all other endocrine organs Most cases of thyroid carcinoma occur between third and seventh decades, but children can also be affected Tumors occur in women 2.5 times more often than in men
- 106. Marc Imhotep Cray, M.D. Thyroid Cancer (2) Investigations 106 Fine-needle biopsy (FNB or FNA [aspiration]) of thyroid nodules makes a diagnosis in most cases Prognosis is a function of morphology of tumor range from a very indolent clinical course to a rapidly fatal disease Radioscintigraphy of gland may help in assessing thyroid tumors hyperfunctioning (“hot”) nodules are usually benign “Cold” or nonfunctioning nodules, more frequently malignant, but may also be benign (i.e., adenoma) Clinical Correlation: Fine-needle Aspiration of Thyroid Nodules Fifteen percent of people have a detectable nodule in thyroid, either by palpation, or by ultrasound imaging Fine-needle aspiration (FNA) is a minimally invasive method to biopsy nodules and screen for rare cases of carcinoma
- 107. Marc Imhotep Cray, M.D. Thyroid Ca (4) Etiopathogenesis 107 Most important environmental factor is external radiation 1. External radiation single most important environmental factor assoc. w increased risk of developing thyroid carcinoma esp. many years of exposure to of high dose 2. Iodine excess and TSH In regions where endemic goiter is widespread, addition of iodine to diet has resulted in increase in incidence of papillary cancer
- 108. Marc Imhotep Cray, M.D. Thyroid Ca (5) Etiopathogenesis 108 3. Genetic basis familial clustering of thyroid cancer has been observed especially in medullary carcinoma Molecular studies reveal thyroid Ca is a multistep process: i. Papillary thyroid carcinoma: mutation in RET gene (overexpression) located on chromosome 10q is seen in about 20% cases of papillary thyroid carcinoma ii. Follicular thyroid carcinoma: About 50% cases of follicular thyroid carcinoma have mutation in RAS family of oncogenes includes H-RAS, N-RAS and K-RAS
- 109. Marc Imhotep Cray, M.D. Thyroid Ca (6) Etiopathogenesis 109 3. Genetic basis familial clustering cont. iii. Medullary thyroid carcinoma: Medullary thyroid carcinoma arises from parafollicular C-cells in thyroid point mutation in RET-proto-oncogene is seen in both familial (MEN2) as a well as sporadic cases of medullary thyroid carcinoma iv. Anaplastic thyroid carcinoma: This tumor either arises from further dedifferentiation of differentiated papillary or follicular thyroid Ca, or by inactivating point mutation in p53 tumor suppressor gene or by mutation in gene coding for β-catenin pathway
- 110. Marc Imhotep Cray, M.D. Thyroid Cancer (7) 110 Major subtypes of thyroid cancer and their relative frequencies are as follows: Papillary carcinoma (more than 85% of cases) Follicular carcinoma (5% to 15% of cases) Medullary carcinoma (5% of cases) Anaplastic (undifferentiated) carcinoma (<5% of cases) Remember genetic markers: Papillary thyroid carcinoma—RET gene Follicular thyroid carcinoma—RAS family of oncogenes Medullary thyroid carcinoma—RET-proto-oncogene Anaplastic thyroid carcinoma—p53 tumor suppressor gene
- 111. Marc Imhotep Cray, M.D. Papillary adenocarcinoma 111 Epidemiology Most common endocrine cancer Papillary carcinoma most common thyroid cancer (>75%) More common in women than men (3:1) o Usually occur in second and third decades Main risk factor: assoc. w radiation exposure Gross and microscopic findings Usually multifocal Papillary leafs intermixed w follicles Psammoma bodies (35–45% of cases) o Dystrophically calcified cancer cells Empty-appearing nuclei o Called Orphan Annie nuclei Lymphatic invasion Metastasize to cervical nodes, lung Diagnose with FNA
- 112. Marc Imhotep Cray, M.D. Papillary carcinoma cont. 112 Treatment Subtotal thyroidectomy w sampling of cervical nodes Followed in a few weeks by radiotherapy w 131I Suppressive therapy w thyroid hormone o Tumor is TSH dependent Five-year survival rate > 95%
- 113. Marc Imhotep Cray, M.D. 113 Rubin R , Strayer DS Eds. Rubin’s Pathology: Clinicopathologic Foundations of Medicine, 6th Ed. Baltimore: Lippincott Williams & Wilkins, 2012. A. Cut surface of a surgically resected thyroid displays a circumscribed pale tan mass w foci of cystic change B. Branching papillae are lined by neoplastic columnar epithelium w clear nuclei A psammoma body is evident (arrow) Papillary carcinoma of thyroid
- 114. Marc Imhotep Cray, M.D. Follicular carcinoma 114 Epidemiology Most common thyroid cancer presenting as a solitary cold nodule Female dominant cancer Gross and microscopic findings Invasion of capsule (distinguishing from follicular adenoma) Neoplastic follicles invade blood vessels Lymph node metastasis is uncommon Metastasize to lung and bone (hematogenous) Treatment similar to papillary cancer Five-year survival rate >80% w treatment
- 115. Marc Imhotep Cray, M.D. 115 Rubin R , Strayer DS Eds. Rubin’s Pathology: Clinicopathologic Foundations of Medicine, 6th Ed. Baltimore: Lippincott Williams & Wilkins, 2012. Evaluating integrity of capsule is critical in distinguishing follicular adenomas from follicular carcinomas: A. In follicular adenomas, a fibrous capsule, usually thin but occasionally more prominent, surrounds neoplastic follicles and no capsular invasion is seen; compressed normal thyroid parenchyma usually is present external to capsule (top) B. In follicular carcinomas demonstrate capsular invasion that may be minimal, as in this case, or widespread, with extension into local structures (vasculature) of neck Capsular invasion in follicular carcinoma
- 116. Marc Imhotep Cray, M.D. Medullary carcinoma 116 Epidemiology Types o Sporadic (80% of cases) o Familial (20% of cases) Familial type o Associated w autosomal dominant MEN IIa/IIb (Sipple syndrome) o MEN IIa syndrome • Medullary carcinoma, hyperparathyroidism (HPTH), pheochromocytoma o MEN IIb (III) syndrome • Medullary carcinoma, mucosal neuromas (lips/tongue), pheochromocytoma (See Endocrinology Tutorial 2_MEN Syndromes) Familial type has a better prognosis than sporadic type Ectopic hormones o ACTH, which can produce Cushing syndrome Male: female ratio is equal
- 117. Marc Imhotep Cray, M.D. 117
- 118. Marc Imhotep Cray, M.D. 118 Pathogenesis Tumors derive from parafollicular C cells C cells synthesize calcitonin o Tumor marker o May produce hypocalcemia o Converted into amyloid can be stained w Congo-red for histologic ID C-cell hyperplasia is a precursor lesion o Calcitonin levels increase w infusion of pentagastrin Diagnosis FNA Serum calcitonin Treatment Total thyroidectomy Genetic screening for familial cases o Detection of mutation of RET proto-oncogene o Thyroidectomy is performed if family member is a gene carrier Medullary carcinoma cont.
- 119. Marc Imhotep Cray, M.D. 119 Medullary thyroid carcinoma. A. Coronal section of a total thyroid resection shows bilateral involvement by a firm, pale tumor. B. The tumor features nests of polygonal cells embedded in a collagenous framework. The connective tissue septa contain eosinophilic amyloid. C. A section stained with Congo red and viewed under polarized light demonstrates the pale green birefringence of amyloid. Rubin R , Strayer DS Eds. Rubin’s Pathology: Clinicopathologic Foundations of Medicine, 6th Ed. Baltimore: Lippincott Williams & Wilkins, 2012.
- 120. Marc Imhotep Cray, M.D. Anaplastic thyroid cancer 120 Epidemiology Most often occurs in elderly women Risk factors o Multinodular goiter, history of follicular cancer Rapidly aggressive and uniformly fatal Treatment o Palliative surgery often compresses trachea o Irradiation or chemotherapy Five-year survival rate is 5%
- 121. Marc Imhotep Cray, M.D. 121 Anaplastic carcinoma of thyroid Rubin R , Strayer DS Eds. Rubin’s Pathology: Clinicopathologic Foundations of Medicine, 6th Ed. Baltimore: Lippincott Williams & Wilkins, 2012. A. tumor in transverse section partially surrounds the trachea and extends into the adjacent soft tissue B. tumor is composed of bizarre spindle and giant cells with polyploid nuclei and numerous mitoses
- 122. Marc Imhotep Cray, M.D. Thyroid Carcinoma Treatment 122 1° treatment for thyroid carcinoma is total thyroidectomy w lymph node dissection depending on tumor stage Radioactive iodine is administered postoperatively to ablate thyroid remnant Anaplastic Ca irradiation or chemotherapy Thyroglobulin (Tg) can then be used as a tumor marker Tg is undetectable in absence of functioning thyroid tissue Rising Tg following 131I ablation indicates recurrence
- 123. Marc Imhotep Cray, M.D. Thyroid Cancer: Key Points 123 Medullary thyroid cancers may occur as an isolated thyroid cancer or may be part of multiple endocrine neoplasia type IIA (MEN IIA) • Medullary thyroid cancers arise from C cells, which secrete calcitonin Other types of thyroid cancer arise from follicular cells Typical triad of MEN IIA is medullary thyroid carcinoma, pheochromocytoma, and primary hyperparathyroidism typical triad of MEN IIB is medullary thyroid carcinoma, pheochromocytoma, and ganglioneuromatosis Typical triad of MEN I is hyperparathyroidism, pancreatic islet cell tumor, and pituitary tumor Both MEN I and MEN II are inherited in an autosomal dominant fashion
- 124. Marc Imhotep Cray, M.D. Vignette # 12 124 A 55-year-old white man presents to the clinic complaining of weakness and fatigue. After taking a detailed history, you learn that he has been suffering from intermittent rectal bleeding and loose stools and that he has lost 15 pounds over the last 2 months. His family history is significant for colon cancer. On physical examination, the patient has marked pallor and a positive stool guaiac test. Laboratory tests reveal an iron deficiency anemia and elevated CEA levels. You schedule a colonoscopy with biopsy for pathologic confirmation of your presumptive diagnosis. What is the Diagnosis?
- 125. Marc Imhotep Cray, M.D. Colorectal Adenocarcinoma 125 Etiology and Epidemiology: Risk factors include adenomatous polyps, long-standing ulcerative colitis, low-fiber diet, old age, positive family history, hereditary nonpolyposis colorectal cancer (HNPCC), and familial adenomatous polyposis (FAP) Most commonly occurs between the ages of 60 and 80 Pathology: Gross: Appearance varies from polypoid mass (proximal colon) to lesions with ulcerated centers and irregular margins that circumscribe bowel (distal colon) Microscopic: Dysplastic columnar cells in glandular formation; may produce mucin, some tumors may be anaplastic
- 126. Marc Imhotep Cray, M.D. Colorectal Ca cont. 126 Clinical Manifestations: Can be asymptomatic; if symptomatic, presents with pallor, weight loss, intermittent diarrhea, LLQ pain, or obstruction Lab findings: Positive stool guaiac test; increased serum CEA; microcytic, hypochromic anemia (iron deficiency anemia secondary to GI bleed) Treatment: Surgical resection; chemotherapy (5-FU) Note: Colorectal cancer is second leading cause of death owing to malignancy U.S. Preventive measures include screening all patients > 50 years of age with colonoscopy every 10 years Colorectal carcinoma - causes, symptoms, diagnosis, treatment, pathology-Osmosis
- 127. Marc Imhotep Cray, M.D. Positive fecal occult blood test 127
- 128. 128 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 129. 129 Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. Philadelphia: Saunders, 2015.
- 131. Marc Imhotep Cray, M.D. Vignette #13 131 A 60-year-old woman presents to the clinic with postmenopausal vaginal bleeding. After taking a complete history, you learn that she is nulliparous and suffers from type 2 diabetes, which is well-controlled with diet and insulin. On physical examination, the woman is obese and has a blood pressure reading of 150/96. You decide to perform a PAP smear as well as an endometrial biopsy. Based on the patient’s presenting signs and medical history, you are worried that you might find well-defined gland patterns lined by malignant stratified columnar epithelial cells on endometrial biopsy. What is the Diagnosis?
- 132. Marc Imhotep Cray, M.D. Endometrial Carcinoma 132 Etiology and Epidemiology: Risk factors include unopposed estrogen use, obesity, diabetes, HTN, nulliparity, and late menopause Peak incidence is between 55 and 65 years of age Endometrial carcinoma is most common gynecologic malignancy Pathology: Typically preceded by endometrial hyperplasia Gross: Localized polypoid tumor or diffuse tumor involving entire endometrial surface Microscopic: Adenocarcinoma characterized by well-defined gland patterns lined by malignant stratified columnar epithelial cells; may see some squamous cells
- 133. Marc Imhotep Cray, M.D. Endometrial Ca. cont. 133 Clinical Manifestations: Presents with postmenopausal vaginal bleeding, leading to early diagnosis; may cause obstruction of cervix with collection of pus (pyometra) or blood (hematometra) presenting with lower abdominal pain Treatment: Total hysterectomy and bilateral salpingo-oophorectomy; radiation therapy Important Note: Endometrial hyperplasia is abnormal endometrial gland proliferation caused by excess estrogen (eg, polycystic ovarian syndrome, estrogen-secreting ovarian tumor, estrogen replacement therapy) It manifests clinically with postmenopausal vaginal bleeding may lead to endometrial cancer depending on degree of atypia
- 134. 134 Endometrial atypical hyperplasia, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 135. 135 Endometrial carcinoma, gross Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 136. 136 Endometrial carcinoma, gross (2) Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 137. 137 Endometrial carcinoma, type I, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 138. 138 Endometrial carcinoma, type II, microscopic Klatt EC. Robbins and Cotran Atlas of Pathology, 3rd Ed. 2015.
- 139. Marc Imhotep Cray, M.D. Colorectal cancer: Key Points 139 Adenocarcinomas make up 98% of primary colon cancers. Precursor lesion to adenocarcinoma is the colonic adenoma, of which the villous type is the most carcinogenic and has the lowest incidence About half of primary colon cancers occur distal to splenic flexure, though this pattern has been changing in recent years Genetics of colon cancer progression are some of the best-studied in oncology • The tumor suppressor gene APC has to sustain two hits before the sequence can continue The next step is usually a mutation of the proto- oncogene KRAS The final step is inactivation of the ubiquitous p53 tumor suppressor gene
- 140. 140 THE END See next slide for links to tools and resources for further study.
- 141. Marc Imhotep Cray, M.D. Further study: 141 eLearning (Cloud) Neoplasia & Oncologic Pathology. Ppt Presentation Oncologic Pathology SDL Tutorial .pdf Atlas: Klatt EC. Robbins and Cotran Atlas of Pathology 3rd Ed. Elsevier- Saunders, 2015. Textbooks: Kumar V and Abbas AK. Robbins Basic Pathology 10th ed. Phil: Saunders, 2018. Rubin R and Strayer DS Eds. Essentials of Rubin's Pathology, 6th Ed.. Baltimore: Lippincott Williams & Wilkins, 2012.