SF 1 School Register
•
12 j'aime•29,856 vues

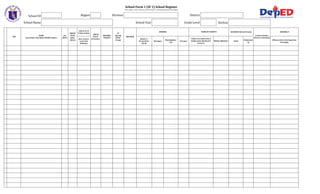
This document is a school register form (SF 1) used to collect student data for a school. It includes fields to record student information such as name, sex, birthdate, address, parents' names, religion, grade level, and remarks. The remarks section codes special designations for students such as those transferred in or out of the school, dropped out, late enrollment, recipients of a CCT program, learners with disabilities, or in accelerated programs. The form is certified by the school adviser and head to verify the accuracy of the student data collected for the school year.

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
Dernier
Dernier (20)
SF 1 School Register
- 1. School Form 1 (SF 1) School Register (This replace Form 1, Master List & STS Form 2-Family Background and Profile) Region School ID Division District School Name LRN NAME (Last Name, First Name, Middle Name) School Year Sex (M/F) BIRTH DATE (mm/ dd/yy) AGE as of 1st Friday of June (nos. of years as per last birthday) BIRTH PLACE (Province) MOTHER TONGUE IP (Specify Ethnic Group) Grade Level ADDRESS NAME OF PARENTS RELIGION House # / Street/Sitio/ Purok Barangay Municipality/ City Section Province Father (1st name only if family name identical to learner) GUARDIAN (If not Parent) REMARK/S Contact Number (Parent /Guardian) Mother (Maiden) Name Relationsh ip (Please refer to the legend on last page)
- 2. LRN NAME (Last Name, First Name, Middle Name) Sex (M/F) BIRTH DATE (mm/ dd/yy) AGE as of 1st Friday of June (nos. of years as per last birthday) BIRTH PLACE (Province) MOTHER TONGUE IP (Specify Ethnic Group) ADDRESS NAME OF PARENTS RELIGION House # / Street/Sitio/ Purok Barangay Municipality/ City Province Father (1st name only if family name identical to learner) List and code of Indicators under REMARK column Indicator Code Required Information Indicator Code Transferred Out T/O Name of Public (P) Private (PR) School & Effectivity Date CCT Recipient Transferred IN T/I DRP LE Name of Public (P) Private (PR) School & Effectivity Date Reason and Effectivity Date Reason (Enrollment beyond 1st Friday of June) Balik-Aral B/A Learner With DissabilityLWD Accelarated ACL Dropped Late Enrollment CCT Required Information BoSY CCT Control/reference number & Effectivity Date FEMALE REMARK/S Contact Number (Parent /Guardian) Mother (Maiden) Name Relationsh ip Prepared by: (Please refer to the legend on last page) Certified Correct: MALE Name of school last attended & Year Specify Specify Level & Effectivity Data EoSY GUARDIAN (If not Parent) TOTAL (Signature of Adviser over Printed Name) Date:___________________________________ (Signature of School Head over Printed Name) Date:__________________________________________________
- 4. _______