Hospital Discharge Process Overview
•Télécharger en tant que PPTX, PDF•
9 j'aime•2,641 vues

Overview of the hospital discharge process as it relates to the development of a new transition of care clinic aimed at reducing the rate of hospital readmissions.

Recommandé
Recommandé
Contenu connexe
Tendances
Tendances (20)
Similaire à Hospital Discharge Process Overview
Similaire à Hospital Discharge Process Overview (20)
Plus de Robert Robinson
Plus de Robert Robinson (11)
Dernier
Dernier (20)
Hospital Discharge Process Overview
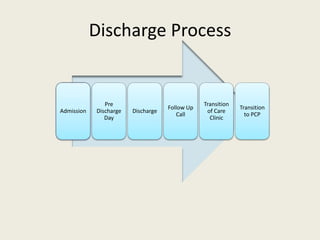
- 1. Discharge Process Admission Pre Discharge Day Discharge Follow Up Call Transition of Care Clinic Transition to PCP
- 2. Discharge Process Timing Admission Pre Discharge Day Discharge Follow Up Call Transition of Care Clinic Transition to PCP Within 2 Working Days of Discharge Within 7 Working Days of Discharge 30 Days Post Discharge
- 3. Discharge Process Admission Pre Discharge Day Discharge Follow Up Call Transition of Care Clinic Transition to PCP
- 4. On Hospital Admission – Part 1 Estimate LOS Progress to Discharge Anticipated Disposition New SNF Placement PT/OT Evaluation Arrange SNF Placement Home or Continued SNF
- 5. On Hospital Admission – Part 2 Progress to Discharge PT/OT Order PT/OT Evaluation Arrange for identified needs Quality Measures Assess for QM Compliance Address QM Needs DME/O2 Order DME/O2 Evaluations Arrange for identified needs Financial SW/PCF Evaluation Arrange for identified needs
- 6. On Hospital Admission - 3 Progress to Discharge Financial SW/PCF Evaluation Arrange for identified needs Education Assess for Educational Needs Address Educational Needs PCP Determine if pt needs PCP Refer to potential PCPs Transportation Determine if pt needs transport Arrange Transport
- 7. Discharge Process Admission Pre Discharge Day Discharge Follow Up Call Transition of Care Clinic Transition to PCP This step ideally starts on the pre-discharge day, but is often combined With discharge day tasks.
- 8. Pre Discharge Day – Part 1 Discharge Is Inpatient Therapy Complete? Disposition Needs Needs Met and Arranged Consultants Follow Up Needed? Arrange for Follow Up Communicate with PCP PCP Notified Flags/Phone Arrange for Follow Up Yes Continue Inpatient Therapy No Process to Discharge
- 9. Pre Discharge Day – Part 2 Discharge Medication Reconciliation MedRec Draft Forms Complete Forms DC Summary Dictate Draft Face to Face Out of Hospital DNR FMLA DME Orders Circle and sign EHR MedRec Quality Measures Recheck Assess for QM Compliance Address QM Needs
- 11. Discharge Day – Part 1 Discharge Medication Reconciliation MedRec Complete Update PCPForms Complete Forms Face to Face Out of Hospital DNR FMLA DME Orders Circle and sign EHR MedRec Final Review Update Consultants Update DC Plans Discharge Orders Complete by 10AM
- 12. Discharge Day – Part 2 Discharge Need Labs for TOCC? Order Labs Discharge PtDC Summary Complete DC Summary Appropriate for TOCC? Schedule for TOCC
- 13. Follow Up Call Admission Pre Discharge Day Discharge Follow Up Call Transition of Care Clinic Transition to PCP
- 14. Phone Call Transitioning to PCP Clinical Status Medication Reconciliation Encourage taking Medications Education Provide needed education Follow Up Confirm Appointments Phone call by hospitalist nurse, MD, or NPP
- 15. Phone Call – Documentation Required • Discharge Date • Working Days past discharge • Summary of phone call • Document in EHR (Centricity/Allscripts)
- 16. Phone Call - Billing • None
- 17. Phone Call - Metrics • Number of eligible patients contacted • Number of tries to contact patient
- 18. Transition of Care Clinic Admission Pre Discharge Day Discharge Follow Up Call Transition of Care Clinic Transition to PCP
- 19. Transition of Care Clinic – Part 1 Transitioning to PCP Clinical Status Education Provide needed education MedRec Update EHRUpdate EHR Update PCP Update Consultants MD or NPP MD, NPP, Pharm MD, NPP, Pharm MD, NPP, or RN
- 20. Transition of Care Clinic – Part 2 Transitioning to PCP Follow Up Confirm Appointments May need repeat TOCC Visit for another E&M Encounter if rapid follow Up cannot be arranged Service Type E&M (All pts) TCM Pts not eligible for TCM if • In Global Surgical Period • TCM Service within 30 days • No phone call • Discharged to SNF • Visit not within 7 working days of DC TCM Patients will have two charges. One for the E&M encounter and one For Transition of Care Management MD or NPP
- 21. TOCC – Documentation Required • Phone Call Data • Working Days post discharge • Coordination of care • Medication reconciliation • E&M Documentation • Document in Centricity/Allscripts
- 22. TOCC Billing • E&M Visit (most if not all patients) • TCM (for TCM eligible patients) • E&M billed immediately • TCM billed 30 days post discharge
- 23. TCM Billing Codes Code Description RVUs Charge 99495 TCM, Moderate Complexity 2.11 $163 99496 TCM, High Complexity 3.05 $231 E&M Billing Codes Code Description RVUs Charge 99214 Office Visit, Est Patient, Level 4 2.21 $100
- 24. TOCC Financial Estimates • Half day of clinic 5 days per week • 3-6 patients per day • 50% qualify for TCM • 2834-5668 RVUs/Year • $162-324k/Year in charges Patients/Week RVU/Week Charges/Week 15 54.5 $3117 30 109 $6234
- 25. Proposed TOCC Metrics • Number of eligible patients served • RVUs • Revenue • 30 Day Readmission rate (TOCC vs non-TOCC) • HCAHPS • PCP Satisfaction
- 26. Transition to PCP Admission Pre Discharge Day Discharge Follow Up Call Transition of Care Clinic Transition to PCP