Tmj and prosthodontic implications
•Download as PPTX, PDF•
122 likes•21,604 views

Temporomandibular joint anatomy and its prosthodontic implications

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (12)
Similar to Tmj and prosthodontic implications
Similar to Tmj and prosthodontic implications (20)
Recently uploaded
Recently uploaded (20)
Tmj and prosthodontic implications
- 1. TEMPOROMANDIBULAR JOINT AND PROSTHODONTIC IMPLICATIONS PRESENTED BY: PRAMOD K CHAHAR 1
- 2. CONTENTS 3 • INTRODUCTION • DEFINITION • PECULIARITY OF TMJ • DEVELOPMENT • ANATOMIC COMPONENTS • VASCULAR SUPPLY TMJ • INNERVATIONS TMJ • MOVEMENTS • PROSTHODONTIC IMPLICATIONS • CONCLUSION • REFERENCES
- 3. 4
- 4. A JOINT is the place of union of two or more bones 5
- 5. A. Fibrous B. Cartilaginous C Synovial JOINTS CAN BE CLASSIFIED AS 6
- 6. DEFINITION OF TMJ • The articulation between the temporal bone and the mandible. It is a bilateral diarthrodial and bilateral ginglymoid joint Glossary of Prosthodontic Terminology-8 7
- 7. TEMPOROMANDIBULAR JOINT IS • Compound • Diarthroidal • Ginglymoid • Multiaxial • Secondary • Squamo-dentary Joint • Cranio–mandibular articulation 8
- 8. PECULIARITY OF TMJ 1. Bilateral diarthrosis 2. Articular surface is formed by fibrous cartilage instead of hyaline cartilage 3. Only joint in human body to have a rigid endpoint of closure 9
- 9. PECULIARITY OF TMJ…… 4. In contrast to other diarthrodial joints TMJ is last joint to develop 5. Develops from two distinct blastema. 10
- 10. DEVELOPMENT OF TMJ At 6th week: Articular disc first appears At 7th week: Meckels cartilage extends from chin to base of skull acts as scaffolding for mandible development Two ectomesenchymal condensation appears At 12th week: Condylar growth cartilage appears & condyle begins to develop 11
- 11. At 22nd week: Articular capsule becomes recognizable and merges peripherally with condensation At 26th week: All components of joint appears except articular eminence At 31st week: Sphenomandibular ligamnet appears At 39th week: Ossification of bony components starts and resembles the future joint DEVELOPMENT OF TMJ…… 12
- 18. BONY COMPONENTS Glenoid fossa Mandibular condyle Articular eminence 20
- 19. - GLENOID FOSSA The squamous portion of the temporal bone (concave ) Measure approx 23 mm (both A-P and M-L) Anterior : a convex bony prominence ( tubercle ) = articular eminence Posterior : Post Glenoid Plane Prevents forced posterior displacement of condyle 21
- 20. The posterior roof is thin not designed to sustain heavy force The articular eminence consists of thick dense bone to tolerate such forces. The steepness of the articular eminence surface dictates the pathway of the condyle CONDYLAR GUIDANCE 22
- 21. THE MANDIBULAR CONDYLE HEAD OF CONDYLE -Mediolateral : 15 – 20 mm -Anteroposterior : 7 – 10 mm -Anterior view : medial & lateral poles, the medial pole more prominent -The actual articulating surface ~ extends anteriorly and posteriorly to the most superior aspect ( P > A ) 23
- 22. The articular surface lies on its anterosuperior aspect, thus facing the posterior slope of the articular eminence of the temporal bone. 24
- 23. 25 The imaginary lines connecting the medial and lateral poles of the condyles are posteriorly and medially directed toward the anterior border of the foramen magnum.
- 24. ARTICULAR EMINENCE Transverse bony bar that forms the root of zygomatic process This articular surface have dense bone and is most heavily traversed by condyle and disk during forward and backward movements of jaw Squamous temporal bone Articular eminence 26
- 25. It is a BICONCAVE FIBROCARTILAGINOUS structure located between the mandibular condyle and the temporal bone. ARTICULAR DISC • The superior surface of the disc SADDLE-SHAPED to fit into the cranial contour, • The inferior surface -CONCAVE to fit against the mandibular condyle. 27
- 26. The ARTICULAR DISC is a roughly oval, firm, fibrous plate. PARTS: 1. ANTERIOR BAND = 2 mm thick 2. POSTERIOR BAND = 3 mm thick, 3. INTERMEDIATE BAND of 1 mm thickness. 28
- 27. • Hinging movements take place in the lower compartment and gliding movements take place in the upper compartment. Larger upper compartment and Smaller lower compartment. 29
- 28. ANTERIORLY: Anterior region of the disc is attached to the capsular ligament Anterio-Superior : anterior margin of the articular surface of the temporal bone -Anterio-Inferior : anterior margin of the articular surface of the condyle ATTACHMENTS OF DISC 31
- 29. POSTERIORLY: RETRODISCAL TISSUE It is a loose connective tissue region that is highly vascularized and innervated. 32
- 30. SUPERIOR : Upper lamina (CONTAINS MAINLY ELASTIC FIBERS) It attaches the disc posteriorly to the tympanic plate & prevents slipping of the disc while yawning. INFERIOR : lower lamina ( COMPOSED CHIEFLY COLLAGENOUS FIBERS ) It prevents excessive rotation of the disc over the condyle. 33
- 31. FUNCTIONS • To accommodate a hinge as well as the gliding actions • Stablize the condyle within TMJ • Articular disc may also reduce wear • Aid lubrication of the joint by storing fluid squeezed out from loaded area 34
- 32. LIGAMENTS Primary 1 Fibrous Capsule 2 Collateral 3 Temporomandibular Acessory 4 Sphenomandibular 5 Stylomandibular 35
- 33. PRIMARY LIGAMENTS 1. CAPSULAR LIGAMENT/ FIBROUS CAPSULE THIN SLEEVE OF FIBROUS TISSUE surrounding the entire TMJ • Superior attachment the borders of the articular surface of the glenoid fossa and anterior edge of preglenoid plane of articular tubercle • Inferior attachment periphery of neck of mandibular condyle 36
- 34. This capsule is reinforced more laterally by an external Temporomandibular ligament, which also limits the distraction and the posterior movement of the condyle. 37
- 35. • Anteriorly, the capsule has an orifice through which the tendon of lateral pterygoid muscle passes. • This area of relative weakness in the capsular lining becomes a source of possible herniation of intra-articular tissues • May allow forward displacement of the disk. 38
- 36. FUNCTION • To resist any lateral or downward forces that tends to separate or dislocate the articular surface • To retain the synovial fluid • Proprioception 39
- 37. COLLATERAL ( DISCAL ) LIGAMENTS • From medial and lateral borders of the disc to the poles of the condyle Medial discal ligament Lateral discal ligament • Dividing the joint mediolaterally into superior and inferior joint cavities 40
- 38. • Permit the disc to be rotated A-P on the articular surface of the condyle • These ligaments are RESPONSIBLE FOR THE HINGING MOVEMENT BETWEEN THE CONDYLE AND THE ARTICULAR DISC • They have a vascular supply and are innervated Function : • Allow the disc to move passively with the condyle as it glides A - P 41
- 39. 3.TEMPOROMANDIBULAR LIGAMENT It lies at the lateral aspect of the capsular ligament Attached above to articular tubercle Below attached to lateral and posterior surface of neck of condyle FUNCTION Resists excessive dropping of the condyle so limits the extent of mouth opening 42
- 40. ACCESORY LIGAMENTS 4.Sphenomandibular ligament From the spine of the sphenoid bone & extends downward to lingula of mandible 43
- 41. 5.Stylomandibular ligament - Second accesory ligament. - This is a specialized dense, local concentration of deep cervical fascia - From the styloid process & extends downward and forward to the angle and posterior border of the ramus of mandible 44
- 42. FUNCTION It limits excessive protrusive movements of the mandible This ligament becomes tense only in extreme protrusive movements. 45
- 44. PRIMARY MUSCLES OF MASTICATION • MASSETER • TEMPORALIS • LATERAL PTERYGOID • MEDIAL PTERYGOID 47
- 48. Voluntary Multipennate Quadrilateral Antigravity Elevator MASSETER 51
- 49. The superficial layer The maxillary process of the zygomatic bone The anterior 2/3rd of the inferior border of the zygomatic arch. The middle layer From the medial aspect of the anterior two-thirds of the zygomatic arch The lower border of the posterior third of this arch The deep layer arises from the deep surface of the zygomatic arch ORIGIN 52
- 50. 53 INSERTION Insert into the angle and lower posterior half of the lateral surface of the mandibular ramus
- 51. Contraction elevates the mandible and brings teeth in contact Provides the force required to chew efficiently Superficial part also helps in protruding Biting foce applied in protruded position ,condyles are stablized against articular eminence by deep fibres FUNCTION OF MASSETER MUSCLE 54
- 52. VASCULAR SUPPLY • By the masseteric branch of the maxillary artery, • the facial artery and • the transverse facial branch of the superficial temporal A INNERVATION By the masseteric branch of the anterior trunk of the mandibular nerve. 55
- 53. TEMPORALIS FAN SHAPED BIPENNATE VOLUNTARY 56
- 54. 57 ORIGIN Arises from the whole of the temporal fossa up to the inferior temporal line and from the deep surface of the temporal fascia. INSERTION Temporalis is attached to the coronoid process and to the anterior border of the mandibular ramus
- 55. Anterior fibers ELEVATION Posterior fibers RETRUSION FUNCTIONS OF TEMPORALIS MUSCLE 58
- 56. VASCULAR SUPPLY The deep temporal branches from the second part of the maxillary artery. INNERVATION The deep temporal branches from the anterior trunk of mandibular nerve 59
- 57. Thick muscle Quadrilateral Multipennate Voluntary MEDIAL PTERYGOID or INTERNAL PTERYGOID Consists 2 heads Deep Head Superficial Head 60
- 58. ORIGIN The large deep head arises from the medial surface of the lateral pterygoid plate of the sphenoid bone The small, superficial head : Maxillary tuberosity and the pyramidal process of the palatine bone INSERTION Postero-inferior part of the medial surface of the ramus and angle of the mandible 61
- 59. FUNCTION: - Contraction - mandible is ELEVATED and the teeth are brought into contact - It is also active in PROTRUDING the mandible - Unilateral contraction - mediotrusive movement of the MANDIBLE 62
- 60. VASCULAR SUPPLY Pterygoid branches of the maxillary artery. INNERVATION Medial pterygoid branch of the mandibular nerve 63
- 61. LATERAL PTERYGOID It consists 2 heads or bellies with different function Superior head Inferior head Thick Short Non-pennate 64
- 62. ORIGIN. The Superior head :Infratemporal surface and :crest of the greater wing of the sphenoid bone. The Inferior head : the lateral surface of lateral pterygoid plate. INSERTION Pterygoid fovea A part of the superior head attached to the capsular ligament and to the anterior and medial borders of articular disc. 65
- 63. FUNCTION : When left and right muscles contract together –protrusive movement If only one lateral pterygoid contracts, the jaw rotates around a vertical axis passing through the opposite condyle and is pulled medially toward the opposite side. During powerful clenching of teeth ,temporalis muscle pulls the condyle backwards which is limited by superior head of lateral pterygoid muscle 66
- 64. Vascular supply Pterygoid branches from the MAXILLARY ARTERY Ascending Palatine branch of FACIAL ARTERY Innervation The superior head & the lateral part of the inferior head: a branch from BUCCAL NERVE. The medial part of the lower head : a branch arising directly from the anterior trunk of MANDIBULAR NERVE.. 67
- 65. BLOOD SUPPLY OF TMJ ARTERIES: Anteriorly: Masseteric A Posteriorly Branches from Maxillary A Superficial temporal A VEINS: Maxillary vein and pterygoid venous plexes 68
- 66. INNERVATION • Movements of synovial joint are initiated & effected by muscle coordination. • Achieved in part through sensory innervation • Branches of the mandibular division of the fifth cranial nerve supply the TMJ • Anterioly by Auriculotemporal and Masseteric Nerve • Posteriolrly by Deep temporal Nerve 69
- 67. MOVEMENTS 70
- 68. CLASSIFICATION 71 HABITUAL Speech Mastication Deglutition Breathing Sucking,whistling etc BASED ON AXIS OF ROTATION Transverse Sagital Vertical LEARNED INNATE
- 69. 72 •BASED ON EXTENT OF MOVEMENT •Border movements •Extreme movements in all planes •Envelope motion •Intra border •Functional •Parafunctional BASED ON TYPE OF MOVEMENT Hinge Protrusive Retrusive Lateral
- 70. AXIS OF MOVEMENTS 73 Transverse or hinge axis: Opening and closing movements takes place in sagital plane Vertical axis: lateral movements takes place through this axis which condyle twists laterally and backward in horizontal plane Antero-posterior or Sagital axis: lateral movements takes place through this axis at which condyle twists while rotating in frontal plane
- 71. All the three axis of mandibular movemnets are inter-related to each other and simultaneous movements occurs around all axis during chewing cycle 74
- 72. MOVEMENTS Rotational / hinge movement in first 20-25mm of mouth opening Translational movement after that when the mouth is excessively opened. 75
- 73. 76
- 74. 77 ACTION OF MASTICATORY MUSCLES ON MANDIBULAR MOVEMENTS
- 75. DEPRESSION OF MANDIBLE Digrastric Geniohyoid Mylohyoid Lateral Pterygoid 78
- 76. ELEVATION OF MANDIBLE Temporalis Medial Pterygoid Masseter 79
- 77. PROTRUSION OF MANDIBLE Lateral Pterygoids Medial Pterygoids 80
- 78. RETRACTION OF MANDIBLE Posterior fibres of Temporalis 81
- 80. 83Teeth must fit into harmony of jaw relationship-not vice -versa
- 81. • The changes in mandible and maxilla occurs slowly over a period of time • Articular surfaces of TMJ undergo slow but continuous remodelling throughout life 84
- 82. 85 VERTICAL DIMENSION Vertical position of mandible in relation to maxilla when teeth are intercuspated at most closed position Dictated by repetitious position of contracted length of elevators
- 83. 86 The vertical dimension determined by contracted length of elevators, sets the limit of jaw separation to which teeth erupts
- 84. CENTRIC RELATION Centric relation is the relationship of the mandible to the maxilla when the properly aligned condyle-disk assemblies are in the most superior position against the eminentiae irrespective of vertical dimension or tooth position GPT 8 87
- 85. HOW MANDIBLE GOES INTO CENTRIC RELATION Triad of strong elevator muscles moves the condyle-disk assembly up on posterior slopes of the articular tubercle The LATERAL PTERYGOID relaxes and stays relaxed during complete closure Complete seating of the condyles in superior most position CENTRIC RELATION 88
- 86. A:SUPERFICIAL MASSETER moves the condyle UP against the posterior slope C:The TEMPORALIS attach to the coronoid process between the teeth and the TMJs and moves THE CONDYLE UP…… B: The MEDIAL PTERYGOID moves THE CONDYLES UP from the lingual side of the mandible 89
- 87. • OCCLUSAL INTERFERENCES Cause • DISPLACEMENT OF TMJ (to achieve max.intercuspation) • Cause INCORDINATION OF MASTICATORY MUSCULATURE • Muscle hyperactivity & PAIN OCCLUSO MUSCLE PAIN 91
- 88. MOST COMMON CONDITIONS AFFECTING TMJ IN A PROSTHETIC SET UP Occlusal discrepencies Dysharmony between centric relation & occlusion Bruxism Emotional stress (mostly in edentulous patients) 92
- 89. OTHER FACTORS AFFECTING TMJ • Trauma • Mal-alignment of the occlusal surfaces of the teeth due to defective crowns or other restorative procedures. . • Excessive gum chewing or nail biting. • Degenerative joint disease, such as osteoarthritis 93
- 90. PRIMARY REQUIREMENTS FOR SUCCESSFUL OCCLUSAL THERAPY • Stable TMJ • Non interfering post.teeth • Anterior teeth in harmony with envelope of function MASTICATORY MUSCLE FUNCTION IS AFFECTED BY THE OTHER 3 STRUCTURES. 94
- 91. TREATMENT 1. Restoration of the occlusal surfaces of the teeth a) Selective reshaping of teeth b) Crown & bridges , Implants 2. Occlusal Splint (also called night guards or mouth guards) 3. Orthodontic treatment & Orthognathic Surgery 95
- 92. A BRIEF ABOUT OCCLUSAL SPLINTS
- 93. OCCLUSAL SPLINTS An occlusal splint is a removable device made of hard acrylic resin creating precise occlusal contact with the teeth of the opposing arch.
- 94. Temporarily provide an orthopedically musculoskeletal stable joint position. Introduces an optimum occlusal condition that prevents the muscular hyperactivity. Used to protect teeth from excessive tooth wear. PRIMARY FUNCTIONS OF OCCLUSAL SPLINTS
- 95. 99 SECONDARY FUNCTION OF OCCLUSAL SPLINTS • Stablization of week teeth • Distribution of occlusal forces • Stablization of unopposed teeth
- 96. TYPES OF OCCLUSAL APPLIANCES THE TWO MOST COMMONLY USED ARE: 1. The Permissive Split 2. The Directive Splint
- 97. INDICATIONS PERMISSIVE SPLINT Stabilizing appliance are generally used to treat muscle pain disorders. (also called as Muscle De-programmer) DIRECTIVE SPLINT Anterior positioning appliance are used to position or align the condyle disk assembly
- 98. The patient is instructed how to properly seat the appliance and the final seating is done by biting. Patients are instructed to wear it in night for bruxism and in day time for disc problems. INSTRUCTIONS
- 99. A splint should be checked at least once during the 1st week after delivery and adjustments are done if required Patients with occlusal splint should preferably be recalled after 3 months months IMPORTANT POINTS IN SPLINT MANAGEMENT
- 100. Dentist must assess the oral function of patients prior to any treatment, since mastication is the most important oral function and it is closely associated with TEMPOROMANDIBULAR JOINT. Therefore, examination of TMJ & thorough knowledge of its anatomy and functioning are the keys for successful PROSTHODONTIC treatment CONCLUSION 104
- 101. REFERENCES.. 1. Strandrings. Grays Anatomy. 40th ed.Elsiever,2008. p530-33 2. Miloro M ,Ghali GE, Larsen P, Waite P, Peterson Editors,Principles of Oral and Maxillofacial Surgery, 2nd Ed.BC Decker Hamilton., 2004 ,p 878-85 3. Dawson PE, Evaluation,Diagnosis and Treatment of Occlusal Problems, 2nd ed, Mosby, 1989, p 18-183 4. Sharry JJ,Complete Denture Prosthodontics, 3rd ed, Blakiston, New York,1974, p 56-100 5. Zarb ,Hobkirk, Eckert, Jacob, et al Editors, ProsthdonticTreatment for Edentulous Patients, 13th ed, Elsiever, 2014 p14-21 6. Stavros Kiliaridis et al ,European Journal of Orthodontics 25 (2003) 259–263 7. International Journal of Applied Dental Sciences 2015; 1(4): 23-26 105
- 102. THANK YOU 106
- 103. 107
Editor's Notes
- THE tmj is a complex joint anatomically and functionally.It is a bilateral, feely movable hinge type of joint, joint is formed by temporal fossa and condyle of mandible, It exhibits two types of movements,rotatory and translatory,there is corelation between occlusion and tmj…and for normal and healthy functionong of this system ,harmony and balance should always be maintained during any type of prosthodontic management..so to maintain this balance we should have thorough knowledge of antomy and functioning of tmj.
- Compound and multi-axial joint,synovial joint,compound joint:in which more than two bones articulates,here articular disc act as third bone
- In reptiles mandible is developed from no; of segmants ,two of these segments quadrate and articulare develops from meckels cartilage so called primary joint or quadra-articulare joint In humans-meckels cartilage give rise to: incus malleus ant ligament of malleus sphenomandibular ligament GINGLYMOID a freely moving joint in which the bones are so articulated as to allow extensive movement in one plane
- This joint cannot independently function on each side ,the movements are synchronized and act together to produce various mandibular movements
- Bony component of jaw Starts developing in membrane as two separate ectomesenchymal condensation between 8-12 weeks in utero
- The most superfi cial layer consists of densely packed fi bres of type I collagen that are arranged mostly parallel to the articular surface. This covers a thin cellular layer, the proliferative zone, that is continuous with the cambial layer of the periosteum beyond the margins of the joint. The third layer, of hypertrophic cartilage, is rich in intercellular matrix: it contains chondrocytes scattered throughout its depth, and randomly oriented fi bres of collagen type II. The fourth layer, immediately above the subchondral bone, is the zone of calcifi cation. Although the number of chondrocytes within the hypertrophic zone decreases with age, undifferentiated mesenchymal cells have been identifi ed in post mortem specimens of all ages (Hansson 1977). This indicates that a capacity for proliferation persists in condylar cartilage, and may be the reason why condylar remodeling occurs throughout life (Robinson 1993,
- The most superfi cial layer consists of densely packed fi bres of type I collagen that are arranged mostly parallel to the articular surface. This covers a thin cellular layer, the proliferative zone, that is continuous with the cambial layer of the periosteum beyond the margins of the joint. The third layer, of hypertrophic cartilage, is rich in intercellular matrix: it contains chondrocytes scattered throughout its depth, and randomly oriented fi bres of collagen type II. The fourth layer, immediately above the subchondral bone, is the zone of calcifi cation. Although the number of chondrocytes within the hypertrophic zone decreases with age, undifferentiated mesenchymal cells have been identifi ed in post mortem specimens of all ages (Hansson 1977). This indicates that a capacity for proliferation persists in condylar cartilage, and may be the reason why condylar remodeling occurs throughout life (Robinson 1993,
- The most superfi cial layer consists of densely packed fi bres of type I collagen that are arranged mostly parallel to the articular surface. This covers a thin cellular layer, the proliferative zone, that is continuous with the cambial layer of the periosteum beyond the margins of the joint. The third layer, of hypertrophic cartilage, is rich in intercellular matrix: it contains chondrocytes scattered throughout its depth, and randomly oriented fi bres of collagen type II. The fourth layer, immediately above the subchondral bone, is the zone of calcifi cation. Although the number of chondrocytes within the hypertrophic zone decreases with age, undifferentiated mesenchymal cells have been identifi ed in post mortem specimens of all ages (Hansson 1977). This indicates that a capacity for proliferation persists in condylar cartilage, and may be the reason why condylar remodeling occurs throughout life (Robinson 1993,
- The most superfi cial layer consists of densely packed fi bres of type I collagen that are arranged mostly parallel to the articular surface. This covers a thin cellular layer, the proliferative zone, that is continuous with the cambial layer of the periosteum beyond the margins of the joint. The third layer, of hypertrophic cartilage, is rich in intercellular matrix: it contains chondrocytes scattered throughout its depth, and randomly oriented fi bres of collagen type II. The fourth layer, immediately above the subchondral bone, is the zone of calcifi cation. Although the number of chondrocytes within the hypertrophic zone decreases with age, undifferentiated mesenchymal cells have been identifi ed in post mortem specimens of all ages (Hansson 1977). This indicates that a capacity for proliferation persists in condylar cartilage, and may be the reason why condylar remodeling occurs throughout life (Robinson 1993,
- E: Articular eminence; ENP: entogolenoid process; t:articular tubercle; Co: condyle; pop: postglenoid process; lb: lateral border of the mandibular fossa; PEP: preglenoid plane; GF: glenoid fossa; Cp: condylar process
- E: Articular eminence; ENP: entogolenoid process; t:articular tubercle; CO: condyle; POP: postglenoid process; LB: lateral border of the mandibular fossa; PEP: preglenoid plane; GF: glenoid fossa; CP: condylar process
- SHAPED like a PEAKED CAP that divides the joint into a It contains 1.2mL of synovial fluid and is responsible for the translational movement of the joint. The inferior compartment has the articular disc as a superior border and the condyle of the mandible as an inferior border. It is slightly smaller with an average synovial fluid volume of 0.9mL and allows rotational movements.
- Anteriorly the disc is also attached by tendinous fibers to the superior lateral pterygoid muscle
- it forms the true posterior boundary of tmj ., the bilaminar region: unlike the rest of the disc, its normal function is to provide attachment rather than intra-articular support.
- Upper lamina- fibro elastic tissue attached to squamotyampanic fissure Lower lamina-fibrous non elastic attached to back side of condyle,prevents excessive rotation of disc over condyle
- The functions of the articular disc remain controversial. It is generally believed that the disc helps to stabilize the condyle within the temporomandibular joint (although see below). The articulating surfaces of the mandibular condyle and the articular fossa fi t together poorly and so are separated by an irregular space. Muscle forces control the position of the mandible, and therefore of the condyle, in relation to the articular eminence, and these in turn determine the shape and thickness of the irregular space. The position of the disc is controlled by neuromuscular forces: the upper head of lateral pterygoid anteriorly, and the elastic tissue in the bilaminar region posteriorly, together pull the disc forward or backward articular disc may also reduce wear, because the frictional force on the condyle and the articular eminence is halved by separating slide and rotation into different joint compartments, aid lubrication of the joint by storing fl uid squeezed out from loaded areas to create a weeping lubricant.
- The broad temporomandibular ligament is attached above to the articular tubercle on the root of the zygomatic process of the temporal bone (Fig. 31.6). It extends downwards and backwards at an angle of approximately 45° to the horizontal, to attach to the lateral surface and posterior border of the neck of the condyle, deep to the parotid gland.
- The sphenomandibular ligament is medial to, and normally separate from, the capsule (Fig. 31.6). It is a fl at, thin band that descends from the spine of the sphenoid and widens as it reaches the lingula of the mandibular foramen.
- The stylomandibular ligament is a thickened band of deep cervical fascia that stretches from the apex and adjacent anterior aspect of the styloid process to the angle and posterior border of the mandible
- consists of three layers which blend anteriorly. The superfi cial layer is the largest. It arises by a thick aponeurosis from the maxillary process of the zygomatic bone and from the anterior twothirds of the inferior border of the zygomatic arch. Its fi bres pass downwards and backwards, to insert into the angle and lower posterior half of the lateral surface of the mandibular ramus. Intramuscular tendinous septa in this layer are responsible for the ridges on the surface of the ramus. The middle layer of masseter arises from the medial aspect of the anterior two-thirds of the zygomatic arch and from the lower border of the posterior third of this arch. It inserts into the central part of the ramus of the mandible. The deep layer arises from the deep surface of the zygomatic arch and inserts into the upper part of the mandibular ramus and into its coronoid process. MULTIPENNATE: MUSCLE WITH MULTIPLE CENTRAL TENDONS TOWARD WHICH MUSCLE FIBRES CONVERGE
- . Its fi bres converge and descend into a tendon which passes through the gap between the zygomatic arch and the side of the skull.
- Its fi bres converge and descend into a tendon which passes through the gap between the zygomatic arch and the side of the skull Temporalis is attached to the medial surface, apex, anterior and posterior borders of the coronoid process and to the anterior border of the mandibular ramus almost upto the third molar tooth
- Medial pterygoid (Fig. 31.12) is a thick, quadrilateral muscle with two heads of origin. The major component is the deep head which arises from the medial surface of the lateral pterygoid plate of the sphenoid bone and is therefore deep to the lower head of lateral pterygoid. The small, superfi cial head arises from the maxillary tuberosity and the pyramidal process of the palatine bone, and therefore lies on the lower head of lateral pterygoid. The fi bres of medial pterygoid descend posterolaterally and are attached by a strong tendinous lamina to the posteroinferior part of the medial surface of the ramus and angle of the mandible
- The fi bres of medial pterygoid descend posterolaterally and are attached by a strong tendinous lamina to the posteroinferior
- Lateral pterygoid (Fig. 31.12) is a short, thick muscle consisting of twoparts. The upper head arises from the infratemporal surface and infratemporal crest of the greater wing of the sphenoid bone. The lower head arises from the lateral surface of the lateral pterygoid plate. From the two origins, the fi bres converge, and pass backwards and laterally, to be inserted into a depression on the front of the neck of the mandible (the pterygoid fovea). A part of the upper head may be attached to the capsule of the temporomandibular joint and to the anterior and medial borders of its articular disc. Unlike the other muscles of mastication, lateral pterygoid is not pennate
- . From the two origins, the fi bres converge, and pass backwards and laterally, into a depression on the front of the neck of the mandible (
- power of a clenching force is due to contractions of masseter and temporalis. The associated backward pull of temporalis is greater than the associated forward pull of (superfi cial) masseter, and so their combined jaw closing action potentially pulls the condyle backward. This is prevented by the simultaneous contraction of the upper head of lateral pterygoid..
- Deep auricular and tympanic art from maxillary art Superficial temporal art
- The mandibular nerve (third branch of the trigeminal nerve) provides the main nerve supply of the TMJ. Additional innervation comes from the masseteric nerve and deep temporal nerves. Parasympathetic fibers of the otic ganglion stimulate the synovial production. Sympathetic neurons from the superior cervical ganglion reach the joint along the vessels and play a role in pain reception and the monitoring of the blood volume.
- Figure a represents the postion of mandibular condyle at rest whre it lies at its superior most postion against posterior slope of glenoid fossa Fig B shows that whwn mandible is opened intially rotation of condyle occurs till 25 mm of mouth opening,here condyle rotates against articular disc and fosa which acts as a single unit Fig C represents the further mouth opening and translation of condyle occurs and here condyle and articular disc as single unit slide sagainst the glenoid fossa figD at the end of translation slight rotation of condyle occurs downward for maximum opening of mouth In fig E closure of mouth starts and condyle rotates upward and traslates in backward direction to seat completely in glenoid fossa
- Dentists must assess the oral function of patients prior to prosthodontic treatment since dental treatment is completed prosthodontically in many cases. Mastication, the most important oral function, is closely associated with temporomandibular joint function. Therefore, examination and diagnosis of temporomandibular joint are the key to success for prosthodontic treatment
- Even though the vertical dimension of occlusion occurs when teeth are fully articulated,the teeth are not determinants ofvertcal dimensionrather it is determined by space available btw fixed maxilla and muscle positioned mandible
- The vertcalthe dimension at maximum intercuspation id determined by muscles regardless of condylar position and when
- Occlusal dysharmony , most common cause of TMD PAIN in patients seeking prosthetic rehabilitation Posterior occlusal interference: When any posterior tooth interferes with the anterior guidance in eccentric movement, the lateral pterygoid muscles are activated and the elevator muscles are hyperactivated. This results in incoordinated muscle hyperfunction. It also puts the posterior teeth in jeopardy of horizontal overload, and subjects them to excessive attritional wear, fractures, and hypermobility.
- Most common cause of masticatory muscle pain is displacement of mandible to a position dictated by maximum intercuspation…which further causes displacement of condyle disc assembly results in changes in alignment of condyle and disc
- (repetitive unconscious clenching or grinding of teeth, often at night). There are many other factors that place undue strain on the TMJ like that place undue strain on the TMJ like
- Comfortable and stable tmj: all occlusal analysis starts with the tmj,the jaw must be able to function and accept loading forces with no discomfort.this is always the starting pointfor any dental trearment that involves the occlusal surface s of teeth Anterior teeth should be in harmony with the envelpoe of functionand also in proper relation with lips,tongue and occlusal plane Non interfering posterior teeth.posterior occlusal contacts should not interfere with either comfortable TMJ in posterior side or anterior guidance in anterior side
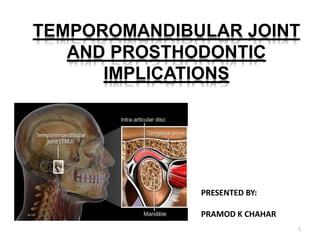
- The temporomandibular joints, called TMJ, are the joints and jaw muscles that make it possible to open and close your mouth. Located on each side of the head, your TMJ work together when you chew, speak or swallow and include muscles and ligaments as well as the jaw bone. They also control the lower jaw (mandible) as it moves forward, backward and side to side. Each TMJ has a disc between the ball and socket. The disc cushions the load while enabling the jaw to open widely and rotate or glide. Any problem that prevents this complex system of muscles, ligaments, discs and bones from working properly may result in a painful TMJ disorder.
- Most common cause of masticatory muscle pain is displacement of mandible to a position dictated by maximum intercuspation even if few microns of interference is present , In order to avoid any unpleasant sensation,the patient will probably not bite on the new dental bridge but rather move his lower jaw into a physiologically unsound position. …which further causes displacement of condyle disc assembly results in changes in alignment of condyle and disc .so the occlusal splint can prevent yhe existing occlusion from controlling jaw to jaw relation at maximum intercuspation An occlusal interference of only few microns can trigger severe irritation. The new bite of convenience causes irregular muscle activity which can eventually lead to temporomandibular joint pain and myalgia
- Unlocks occlusion-prevents occlusal interferences and cause the muscle to relax and seating of condyles in centric relaton and eleminates the muscle incordination A permissive (smooth) anterior splint separates the interfering Molar from contact, thus permitting the condyle disk assemblies to Seat up into centric relation. This eliminates the trigger for muscle activity And allows the inferior lateral pterygoid muscle to release. Peaceful, comfortable muscle activity resumes quickly.