Calcium homeostasis vitamin d-parathyroid-calcitonin role (rickets,hypercalcemia,hyperparathyroidism,osteoporosis,renal osteodystrophy) prevention dr.sandeep c agrawal agrasen hospital gondia india
•Télécharger en tant que PPTX, PDF•
47 j'aime•5,719 vues

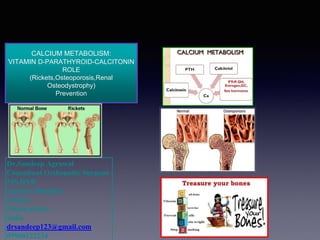
CALCIUM METABOLISM: VITAMIN D-PARATHYROID-CALCITONIN ROLE (Rickets,Osteoporosis,Renal Osteodystrophy) Prevention Dr.Sandeep C Agrawal Agrasen Hospital Gondia India Metabolic Bone Diseases:phosphorus,magnesium and other minerals ,Calcium and vitamin D rich diets,Sunlight exposure,vitamin D synthesis,Osteoporosis prevention and diet

Recommandé
Contenu connexe
Tendances
Tendances (20)
En vedette
En vedette (10)
Similaire à Calcium homeostasis vitamin d-parathyroid-calcitonin role (rickets,hypercalcemia,hyperparathyroidism,osteoporosis,renal osteodystrophy) prevention dr.sandeep c agrawal agrasen hospital gondia india
Similaire à Calcium homeostasis vitamin d-parathyroid-calcitonin role (rickets,hypercalcemia,hyperparathyroidism,osteoporosis,renal osteodystrophy) prevention dr.sandeep c agrawal agrasen hospital gondia india (20)
Plus de AGRASEN Fracture Arthritis Hospital, Ganesh Nagar,Gondia,Maharashtra,INDIA
Plus de AGRASEN Fracture Arthritis Hospital, Ganesh Nagar,Gondia,Maharashtra,INDIA (20)
Dernier
Dernier (20)
Calcium homeostasis vitamin d-parathyroid-calcitonin role (rickets,hypercalcemia,hyperparathyroidism,osteoporosis,renal osteodystrophy) prevention dr.sandeep c agrawal agrasen hospital gondia india
- 1. Dr.Sandeep Agrawal Consultant Orthopedic Surgeon MS,DNB Agrasen Hospital Gondia Maharashtra India drsandeep123@gmail.com 09960122234 CALCIUM METABOLISM: VITAMIN D-PARATHYROID-CALCITONIN ROLE (Rickets,Osteoporosis,Renal Osteodystrophy) Prevention
- 2. NORMAL VALUES Total body calcium – 1100 g {27.5 mol / L} 99 % in bones Plasma calcium : 9 – 11 mg / dL {5 m Eq / L or 2.5 mmol / L} Ionized calcium – 50 % {1.2 mmol / L} Protein bound – 41 % {1.0 mmol / L} Complexed with anions – 9 % {0.2 mmol / L}
- 3. 3
- 4. • PRINCIPLE ORGAN SYSTEMS • GUT, BONE, KIDNEYS – HORMONES • PARATHYROID HORMONE (PTH), VITAMIN D,CALCITONIN BLOOD CALCIUM REGULATION
- 5. GLOMERULAR FILTRATE 250 mmol DIET 25mmol (1000 mg) GIT FECES 22.5mmol ABSORPTION 15 mmol SECRETION 12.5 mmol REABSORPTION 247.5 mmol ECF 35 mmol URINE 2.5 mmol BONE EXCHANGEABLE 100 mmol STABLE 27,200 mmol RAPID EXCHANGE 500 mmol REABSORPTION 7.5 mmol
- 6. 1. Rapid phase – osteolysis by osteocytes 2. Slow phase – by osteoclasts
- 7. CALCIUM PHYSIOLOGY: BLOOD CALCIUM CALCIUM FLUX INTO AND OUT OF BLOOD: “IN” FACTORS: INTESTINAL ABSORPTION, BONE RESORPTION “OUT” FACTORS: RENAL EXCRETION, BONE FORMATION (Ca INCORPATION INTO BONE) BALANCE BETWEEN “IN” AND “OUT” FACTORS ORGAN PHYSIOLOGY OF GUT, BONE, AND KIDNEY HORMONE FUNCTION OF PTH AND VITMAMIN D 1. Neutral – normal healthy adults – daily intake & excretion same – bone entry & exit same 2. Positive – growing children – intestinal absorption > excretion – bone entry > bone exit 3. Negative – pregnant & lactating women - intestinal absorption < excretion – bone entry < bone exit “CALCIUM BALANCE”
- 8. CALCIUM HOMEOSTASIS DIETARY CALCIUM INTESTINAL ABSORPTION ORGAN PHYSIOLOGY ENDOCRINE PHYSIOLOGY DIETARY HABITS, SUPPLEMENTS BLOOD CALCIUM BONE KIDNEYS URINE THE ONLY “IN” THE PRINCIPLE “OUT” ORGAN PHYS. ENDOCRINE PHYS. ORGAN, ENDOCRINE
- 11. CALCIUM, PTH, AND VITAMIN D FEEDBACK LOOPS NORMAL BLOOD Ca RISING BLOOD Ca FALLING BLOOD Ca SUPPRESS PTH STIMULATE PTH BONE RESORPTION URINARY LOSS 1,25(OH)2 D PRODUCTION BONE RESORPTION URINARY LOSS 1,25(OH)2 D PRODUCTION
- 12. FUNCTIONS OF CALCIUM Blood coagulation Muscle contraction Transmission of nerve impulses Formation of skeleton ,etc. FREE IONIZED CALCIUM
- 13. CALCIUM IN GIT • 30 – 80 % of ingested calcium is absorbed • Actively transported out of the intestinal cells with the help of Ca 2+ dependent ATPase • Increased plasma calcium – decreased absorption from the gut • Decreased by phosphates and oxalates and alkalis • Increased by high protein diet 1,25 Vitamin D3
- 15. CALCIUM IN KIDNEYS • 98 % - 99 % is reabsorbed 60 % in PCT 40 % in Ascending limb of LOH Distal tubule PARATHYROID HORMONE
- 16. RECOMMENDED DAILY INTAKE OF VITAMIN D ESTIMATED DAILY CALCIUM INTAKES
- 20. Calcium Citrate
- 23. NORMAL VALUES • Total body phosphate – 500 to 800 g. • 85 – 90 % in skeleton • Plasma phosphate – 12 mg / dL 2/3rd – organic 1/3rd – inorganic {Pi} ex. PO4 3- , HPO4 2-, H2PO4 2- FUNCTIONS ATPase , c AMP , 2-3, DPG Phosphorylation and Dephosphorylation PHOSPHATE METABOLISM
- 24. Phosphate is found in ATP, DNA, RNA, cAMP, 2,3-DPG, many proteins. Phosphorylation and dephosphorylation of proteins are involved in the regulation of cell function – bone - buffer Inorganic phosphate in the plasma is mainly in two forms: HPO4- (1.05 mmol/L) and H2PO4- (0.26 mmol/L) pH of the ECF becomes more acidic, Relative increase in H2PO4- and a decrease in HPO4- and viceversa. Decreasing level of phosphate in ECF from far below normal does not cause major immediate effects on the body. In contrast, even slight increases or decreases of calcium ion in ECF can cause extreme immediate physiologic effects. chronic hypocalcemia or hypophosphatemia greatly decreases bone mineralization
- 25. BONE SALTS • Salts of calcium and phosphate. HYDROXYAPATITE Ca10(PO4)6. (OH)2 400 Å long 10 – 30 Å thick 100 Å wide Ca / P ratio – 1.3 to 2.0 Other salts: Mg2+, Na+ , K+ ions conjugated to bone crystals.
- 26. BONE: 3 mg of PO4 enters and is again reabsorbed. KIDNEYS: 85 % - 90 % of filtered Pi is reabsorbed by Active Transport in PCT PTH Overflow mechanism Phosphorus
- 27. G I T • Absorbed in duodenum and small intestine by Active transport and passive diffusion. • Absorption is linear to dietary intake.
- 28. VITAMIN D PHYSIOLOGYFORMATION OF VITAMIN D3
- 29. – 25-HYDROXYLASE FUNCTIONS CONSTITUTIVELY WITHOUT INPUT FROM BLOOD CALCIUM STATUS OR PTH – 25(OH)VITAMIN D IS THE BEST SCREENING TEST FOR VITAMIN D ADEQUACY VITAMIN D RESISTANT RICKETS: mutations in the gene coding for the enzyme 1 α HYDROXYLASE
- 30. calcium homeostasis absorption of Ca and P in the small intestine Role of vitamin D normal mineralization of bone reabsorption Ca and P in the renal tubule
- 33. • THE COUPLED PROCESS OF BONE TURNOVER CAN BE MEASURED BY: – MARKERS OF OSTEOBLAST METABOLISM • SERUM BONE-SPECIFIC ALKALINE PHOSPHATASE • SERUM OSTEOCALCIN – MARKERS OF OSTEOCLAST METABOLISM • URINE PRODUCTS OF BONE COLLAGEN BREAKDOWN – HYDROXYPROLINE – N-TELOPEPTIDES – PYRIDINIUM CROSSLINKS MEASUREMENT OF BONE TURNOVER
- 34. Vitamin D Intake of vitamin D3 can increase many times and yet the concentration of 25- hydroxycholecalciferol remains nearly normal - prevents excessive action of vitamin D conserves the vitamin D stored in the liver for future use. Once it is converted, it persists in the body for only a few weeks, whereas in the vitamin D form, it can be stored in the liver for many months.
- 35. When the plasma calcium concentration is too high, the formation of 1,25-dihydroxycholecalciferol is greatly depressed – decreases the absorption of calcium from the intestines, the bones, and the renal tubules. z
- 36. Serum 25(OH)D (calcidiol) vitamin D - Normal potential deficiency-insufficiecy adverse effects 0 25 50 75 125 nmol/L ** 1 nmol/L = 0.4 ng/mL ≥50 nmol/L (≥20 ng/mL) >125 nmol/L (>50 ng/mL)
- 37. • EXCESSIVE INTAKE OF VITAMIN D – RELATIVELY HARD TO DO IF ALL RELEVANT ORGAN SYSTEMS ARE FUNCTIONING PROPERLY; GENERALLY REQUIRES PRESCRIPTION STRENGTH VITAMIN D, PARTICULARLY 1,25(OH)2D (CALCITRIOL) • EXCESSIVE PRODUCTION OF 1,25(OH)2D – EXTRA-RENAL 1-HYDROXYLATION OF 25(OH)VITAMIN D BY AN ENZYME WITH 1-HYDROXYLASE ACTIVITY, WHICH IS DISTINCT FROM RENAL ENZYME • USUALLY ASSOCIATED WITH GRANULOMAS (MACROPHAGES) OR ABNORMAL LYMPHOID TISSUE (B CELL LYMPHOMA) • NOT REGULATED BY PTH OR CALCIUM HYPERVITAMINOSIS D
- 39. ACTIONS OF PTH I. Increases calcium and phosphate absorption from the bones II. Decreases excretion of calcium by the kidneys III. Increases the excretion of phosphate by the kidneys IV. Increases intestinal absorption of calcium and phosphate. INCREASED PLASMA CALCIUM
- 42. PTH - Kidneys 1. PTH causes rapid loss of phosphate in urine owing to the effect of the hormone to diminish proximal tubular reabsorption of phosphate ions. PHOSPHATURIC ACTION 2.PTH increases renal tubular reabsorption of Ca. 3. increases reabsorption of Mg ions and H ions 4.decreases reabsorption of Na, K and amino acid No PTH - continual loss of Ca into the urine would eventually deplete both the ECF and the bones
- 47. • STIMULUS : Increased plasma calcium Others: β adrenergic agonists, dopamine and estrogen, GASTRIN, CCK, glucagon.. • ACTIONS: Decreases absorptive action of osteoclasts Deposits exchangeable Ca in bone salts Decreases the formation of osteoclasts • CLINICAL USE: Used in the treatment of PAGET’S DISEASE. CALCITONIN
- 48. RICKETS
- 49. RICKETS
- 50. Rickets leads to cupping and to a brush−like appearance of the epiphyseal ends on radiograms. Radiographs of the knee of a 3.6-year- old girl with hypophosphatemia depict severe fraying of the metaphysis. N Active Rickets recovery
- 53. 53 OSTEOPOROSIS
- 54. • SKELETAL MASS IN HUMAN REACHES A PEAK AT ABOUT AGE 30 – BEFORE 30 : – SKELETAL MASS INCREASING.. – BONE FORMATION EXCEEDS BONE RESORPTION. – AT 30: – TWO PROCESSES ARE EXACTLY MATCHED – AFTER 30: – SKELETAL MASS IS LOST FOR THE REST OF LIFE
- 55. Normal bone has the appearance of a honeycomb matrix (left). Under a microscope, osteoporotic bone (right) looks more porous.
- 57. • Bone mineral density (BMD) is the current measure (major determinant) of fracture risk. (Not DEXA) WHO criteria • Mean for age – T score: 0 • Osteopenia – T score: -1.0~- 2.5 • Osteoporosis – T score < -2.5 Incidence of Fem neck fx (A) and Intertrochanteric fx (B) by BMD Osteoporosis
- 58. What keeps bones healthy Regular exercise Adequate amounts of calcium Adequate amounts of vitamin D, which is very essential for absorbing calcium
- 63. TESTS AND DIAGNOSIS Osteopenia refers to mild bone loss that isn't severe enough to be called osteoporosis, but that increases the risk of osteoporosis. The best screening test is dual energy X-ray absorptiometry (DEXA) – measures the density of bones in the spine, hip and wrist and it's used to accurately follow changes in these bones over time. Ultrasound Quantitative CT scanning Dual energy X-ray absorptiometry
- 66. ThanksPersistence in your presentations, this is one secret to success. After my first presentation, I got up and did it again. Even though I was scared to death, I did it again. So preparation in all areas of life is so vital to your success. Don’t be lazy in preparing; don’t be lazy in laying the groundwork that will make all of the difference in how your life turns out. What you may be lacking in are the strong feelings about what you want and what you want to do. Let these strong feelings help you take a second look at your life. After all, you’ve only got one life, at least on this planet. So why not make it an adventure in achievement? Why not discover what all you can do and what all you can have? Why not now take the Challenge to Succeed! First you need to succeed to survive. We must take the seasons and learn how to use them with the seed, the soil and the rain of opportunity to learn how to sustain ourselves and our family. But then second is to then succeed to flourish in every part of your life today than yesterday, in our speech, our language, our health, everything we can possibility think of.
- 67. This presentation is for doctors and students in general. . Graphics,Images and jpeg files are taken from Google and yahoo Image to heighten the specific points in this presentation. • If there is any objection/or copyright violation, please inform drsandeep123@gmail.com for prompt deletion. • It is intended for use only by the doctors of orthopaedic surgery. . Views expressed in this presentation are personal. • .For any confusion please contact the sole author for clarification. • Every body is allowed to copy or download and use the material best suited to him. There is no financial involvement. • For any correction or suggestion please contact drsandeep123@gmail.com.