Improving the Recognition and Management of Amyloid-Related Imaging Abnormalities (ARIA) in Alzheimer’s Disease Treatment: Practical Tools & Strategies for Radiology & Neuroradiology Specialists
•
0 j'aime•25 vues

Co-Chairs, Jerome A. Barakos, MD, and Tammie L.S. Benzinger, MD, PhD, prepared useful Practice Aids pertaining to Alzheimer's disease for this CME/AAPA activity titled “Improving the Recognition and Management of Amyloid-Related Imaging Abnormalities (ARIA) in Alzheimer’s Disease Treatment: Practical Tools & Strategies for Radiology & Neuroradiology Specialists.” For the full presentation, downloadable Practice Aids, and complete CME/AAPA information, and to apply for credit, please visit us at https://bit.ly/48NS10t. CME/AAPA credit will be available until March 14, 2025.

Recommandé
Recommandé
Contenu connexe
Similaire à Improving the Recognition and Management of Amyloid-Related Imaging Abnormalities (ARIA) in Alzheimer’s Disease Treatment: Practical Tools & Strategies for Radiology & Neuroradiology Specialists
Similaire à Improving the Recognition and Management of Amyloid-Related Imaging Abnormalities (ARIA) in Alzheimer’s Disease Treatment: Practical Tools & Strategies for Radiology & Neuroradiology Specialists (20)
Plus de PVI, PeerView Institute for Medical Education
Plus de PVI, PeerView Institute for Medical Education (20)
Dernier
Dernier (20)
Improving the Recognition and Management of Amyloid-Related Imaging Abnormalities (ARIA) in Alzheimer’s Disease Treatment: Practical Tools & Strategies for Radiology & Neuroradiology Specialists
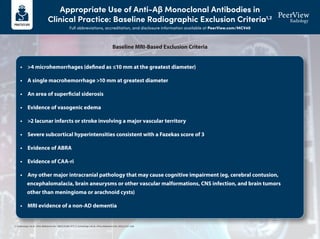
- 1. Appropriate Use of Anti-Aβ Monoclonal Antibodies in Clinical Practice: Baseline Radiographic Exclusion Criteria1,2 Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 1. Cummings J et al. J Prev Alzheimers Dis. 2023;10:362-377. 2. Cummings J et al. J Prev Alzheimers Dis. 2022;2:221-230. • >4 microhemorrhages (defined as ≤10 mm at the greatest diameter) • A single macrohemorrhage >10 mm at greatest diameter • An area of superficial siderosis • Evidence of vasogenic edema • >2 lacunar infarcts or stroke involving a major vascular territory • Severe subcortical hyperintensities consistent with a Fazekas score of 3 • Evidence of ABRA • Evidence of CAA-ri • Any other major intracranial pathology that may cause cognitive impairment (eg, cerebral contusion, encephalomalacia, brain aneurysms or other vascular malformations, CNS infection, and brain tumors other than meningioma or arachnoid cysts) • MRI evidence of a non-AD dementia Baseline MRI-Based Exclusion Criteria
- 2. Detecting, Monitoring, and Managing Amyloid-Related Imaging Abnormalities (ARIA) Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 3T scanner (recommended) 1.5T scanner (minimal) High field strength scanners have greater sensitivity but limited availability The use of 1.5T scanner is endorsed as a minimum standard Slice thickness: ≤5 mm Thinner slices increase resolution, but decrease signal-to-noise ratio TE: ≥20 ms Longer TE increases sensitivity to detection 2D T2* GRE or SWI (for ARIA-H) MRI sequences used to improve the detection, visualization, and monitoring of microhemorrhages and superficial siderosis (ARIA-H) T2-FLAIR (for ARIA-E) MRI sequences used to detect and monitor brain edema or sulcal effusion (ARIA-E) Diffusion-weighted imaging An MRI method used to differentiate between ARIA and cytotoxic processes (eg, infarcts) Recommended for differential diagnosis Visit the American Society for Neuroradiology (ASNR) website to access ARIA resources, including links to standardized protocols for 3T and 1.5T scanners via this QR code or URL: https://www.asnr.org/education-resources/alzheimers-webinar-series MRI Acquisition Protocols to Detect and Monitor ARIA1-3
- 3. Detecting, Monitoring, and Managing Amyloid-Related Imaging Abnormalities (ARIA) Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 ARIA Type ARIA-E ARIA-H microhemorrhage ARIA-H superficial siderosis FLAIR hyperintensity confined to sulcus and/or cortex/subcortical white matter in one location <5 cm Mild Moderate Radiographic Severity Severe ≤4 new incident microhemorrhages One focal area of superficial siderosis FLAIR hyperintensity 5-10 cm, or more than one site of involvement, each measuring <10 cm 5-9 new incident microhemorrhages Two focal areas of superficial siderosis FLAIR hyperintensity measures >10 cm, often with significant subcortical white matter and/or sulcal involvement; ≥1 separate sites of involvement might be noted ≥10 new incident microhemorrhages >2 focal areas of superficial siderosis Classifying ARIA by Radiographic Severity4,5
- 4. Detecting, Monitoring, and Managing Amyloid-Related Imaging Abnormalities (ARIA) Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 Headache Confusion and dizziness Neuropsychiatric symptoms Nausea Gait disturbance Visual disturbance/ blurred vision Seizure Less frequent Uncommon Symptom Severity Mild Discomfort noted; no disruption of daily activity Moderate Discomfort sufficient to reduce or affect normal daily activity Severe Incapacitating, with inability to perform normal daily activity Symptoms Consistent With ARIA That Should Trigger Out-of-Sequence MRI6-8
- 5. Detecting, Monitoring, and Managing Amyloid-Related Imaging Abnormalities (ARIA) Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 Baseline MRI has no exclusion factors MRI routine or conducted because of symptoms suggestive of ARIA ARIA-E or ARIA-H detected Symptomatic Asymptomatic Radiographically mild ARIA-E or mild ARIA-H Continue treatment with anti-Aβ antibody; monthly MRI Continue treatment; discontinue monthly MRI if ARIA-E resolves or ARIA-H stabilizes Resume treatment with anti-Aβ antibody Suspend treatment; clinical assessment; repeat MRI monthly Radiographically moderate/severe ARIA-E or moderate/severe ARIA-H MRI shows resolution of ARIA-E or stabilization of ARIA-H; symptoms resolve; patient wishes to continue Stop anti-Aβ antibody therapy for any of the following • Any macrohemorrhage • >1 area of superficial siderosis • >10 microhemorrhages since treatment initiation • >2 episodes of ARIA • Severe symptoms of ARIA • Patient requires treatment with an anticoagulant Severity of Changes Observed on MRI Radiographic ARIA-E: Mild Radiographic ARIA-E: Moderate Radiographic ARIA-E: Severe Radiographic ARIA-H: Mild Radiographic ARIA-H: Moderate Radiographic ARIA-H: Severe Symptom Description No Symptoms Mild Symptoms Moderate Symptoms Severe Symptoms Discontinue dosing Discontinue dosing Discontinue dosing Discontinue dosing Discontinue dosing Discontinue dosing Discontinue dosing Discontinue dosing Discontinue dosing Discontinue dosing Suspend dosing Suspend dosing Suspend dosing Suspend dosing Suspend dosing Suspend dosing Suspend dosing Suspend dosing Suspend dosing Suspend dosing Discontinue dosing Discontinue dosing Continue dosing Continue dosing ARIA Management Algorithm6-8 1. Cogswell PM et al. AJNR Am J Neuroradiol. 2022;43:E19-E35. 2. Sperling RA et al. Alzheimers Dement. 2011;7:367-385. 3. Barakos J et al. J Prev Alzheimers Dis. 2022;9:211-220. 4. Aduhelm (aducanumab) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761178s007lbl.pdf. 5. Leqembi (lecanemab) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761269s000lbl.pdf. 6. Cummings J et al. J Prev Alzheimers Dis. 2023;10:362-377. 7. Cummings J et al. J Prev Alzheimers Dis. 2022;2:221-230. 8. Cummings J et al. J Prev Alzheimers Dis. 2021;4:398-410.
- 6. Selected Images of Amyloid-Related Imaging Abnormalities (ARIA) and Its Mimics Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 Parenchymal Edema New T2-FLAIR hyperintense signal with mild local mass effect and sulcal effacement measuring <5 cm (mild ARIA-E) New multifocal, patchy T2-FLAIR hyperintense signal, each region measuring <5 cm (moderate ARIA-E); multiple ARIA-E yields a classification of moderate, as long as each region is <10 cm Extensive T2-FLAIR hyperintense signal throughout the right frontal and parietal lobes measuring >10 cm (severe ARIA-E); associated mass effect and sulcal effacement throughout much of the right hemisphere Baseline Baseline Baseline Post-treatment Post-treatment Post-treatment Mild Moderate Severe New sulcal T2-FLAIR hyperintense signal measuring <5 cm in transverse dimensions (mild ARIA-E) New T2-FLAIR sulcal effusion involving the right posterior temporal and parietal lobes measuring 5-10 cm (moderate ARIA-E) Extensive T2-FLAIR sulcal effusion involving the bilateral temporal and occipital lobes measuring ≥10 cm in extent (severe ARIA-E) Baseline Post-treatment Mild Sulcal Effusion Baseline Post-treatment Moderate Baseline Post-treatment Severe ARIA-E Examples (Detected With T2-FLAIR Sequence)1
- 7. Selected Images of Amyloid-Related Imaging Abnormalities (ARIA) and Its Mimics Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 Microhemorrhage Postdosing, ≥10 new microhemorrhages (severe ARIA-H) Baseline Post-treatment Severe Postdosing, 5 treatment-emergent microhemorrhages (moderate ARIA-H) Baseline Post-treatment Moderate Postdosing, few (<5) new peripheral left frontal microhemorrhages (mild ARIA-H) Baseline Post-treatment Mild Superficial Siderosis Postdosing, new right temporal superficial siderosis, which involves contiguous sulci when viewed over multiple slices (mild ARIA-H, siderosis); this patient also had two treatment-emergent microhemorrhages (mild ARIA-H, microhemorrhage) Two regions of treatment-emergent superficial siderosis in the right greater-than-left frontal lobes (moderate ARIA-H) Baseline Post-treatment Mild Baseline Post-treatment Moderate ARIA-H Examples (Detected With T2-GRE or SWI Sequence)1
- 8. Selected Images of Amyloid-Related Imaging Abnormalities (ARIA) and Its Mimics Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 Infarct (Early Subacute) FLAIR+ (hyperintensity) • In addition to FLAIR and GRE/SWI sequences, a trace DWI sequence should be included as routine protocol in ARIA monitoring examinations to help with the differential diagnosis of new signal abnormalities • For example, the DWI sequence plays an important role in helping to differentiate ARIA-E from potential cytotoxic edema caused by an incidental infarct • In classic cases of ARIA, the diffusion restriction will be absent, because intense diffusion restriction associated with an infarct is not a characteristic of ARIA • The DWI sequence helped to identify the underlying etiology of this patient’s radiographic findings • Diffusion restriction was identified, which indicated that it was not ARIA • However, the diffusion restriction was located in the sulci, which is not a typical pattern seen with acute or subacute infarcts • This patient was diagnosed with bacterial meningitis following confirmatory lab testing Infection (Bacterial Meningitis) FLAIR+ (vasogenic edema and sulcal effusions) GRE/SWI+ (microhemorrhages and superficial siderosis) DWI+ (with restricted diffusion in the sulci) DWI+ (with restricted diffusion) GRE/SWI+ (microhemorrhage) ARIA Mimics2
- 9. Selected Images of Amyloid-Related Imaging Abnormalities (ARIA) and Its Mimics Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 1. Cogswell PM et al. Am J Neuroradiol. 2022;43:E19-E35. 2. Images courtesy of Tammie L.S. Benzinger, MD, PhD. ARIA Mimics2 Brain Metastasis FLAIR+ (hyperintensity) • New signal abnormalities detected in ARIA monitoring examinations may require T1-weighted gadolinium-enhanced imaging to differentiate between ARIA and brain metastases • Contrast-enhanced imaging should be considered based on the patient’s medical history and/or any clinical findings that may suggest the possibility of a metastatic etiology • ARIA and PRES are usually indistinguishable based on MRI (eg, both will typically have FLAIR hyperintensities and no restricted diffusion) • Therefore, the clinical context is critical to differentiate between ARIA and PRES • This patient presented to the emergency department with confusion, headache, and very high blood pressure (which is a classic presentation for PRES) • They were treated for their hypertension, which resolved their clinical symptoms and their edema Posterior Reversible Encephalopathy Syndrome (PRES) FLAIR+ (hyperintensities) GRE/SWI negative DWI negative (no diffusion restriction) T1 postcontrast + enhancement GRE/SWI+ (microhemorrhage) T1 postcontrast
- 10. Use the following pages as reporting templates to document baseline screening MRI prior to initiating anti-amyloid therapy (page 1) and follow-up MRI to monitor ARIA in patients undergoing treatment with anti-amyloid therapy (pages 2-3). Printable Resource ARIA Reporting Templates Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40
- 11. Baseline MRI for Screening Prior to Initiating Anti-Amyloid Therapy (page 1 of 1) Scan Information (fill in or circle response as needed) DWI Gadolinium Contrast ARIA–H Sequence ARIA–E Sequence Slice Gap Slice Thickness (mm) Field Strength Model Manufacturer Y N Y N SWI GRE/T2* 3D T2-FLAIR 1.5T 3T Hyperintensities/Infarcts Summary Location (eg, frontal, parietal, occipital, temporal, brainstem, cerebellum) L/R Type (eg, parenchymal; sulcal) Max Diameter (cm) Lesion 1 Lesion 2 Lesion 3 Lesion 4 Microhemorrhages/Superficial Siderosis Summary Brainstem Deep Gray Cerebellum Temporal Frontal Parietal Occipital Total MCH count SS count Findings Total FLAIR hyperintensities: ______________ Describe locations and measure longest size in 1 dimension for each: _________________________________________________________________ Total microhemorrhages: ________________ Describe locations in general, deep vs lobar: ____________________________________________________________________________________ Total areas of superficial siderosis: __________________ Describe locations: _________________________________________________________________________________________________________ General description of other acute or chronic findings (eg, macrohemorrhage >10 mm; vasogenic edema; >2 lacunar infarcts or stroke involving a major vascular territory; severe subcortical hyperintensities consistent with a Fazekas score of 3; evidence of ABRA; evidence of CAA-ri; evidence of non-AD dementia; any other major intracranial pathology that may cause cognitive impairment): _____________________________________________________________________________________________________________________________ _____________________________________________________________________________________________________________________________ IMPRESSION Total microhemorrhages (circle one): 0-4 5-9 ≥10 Superficial siderosis (circle one): is not detected is present Note any other EXCLUSION CRITERIA for initiating treatment with anti-amyloid therapy: ____________________________________________________________________________________________________________________ Restricted Diffusion (circle correct response) Contrast Enhancement (circle correct response) Yes No N/A Yes No N/A Patient Information Patient name:____________________________ Age:________ Sex:_______ Patient ID:___________________ Referring MD:________________________ Report Information Scan Date:_________________________________ Site Location:_______________________________ Updated findings were conveyed to _____________________________ by _______________________________ (referring physician) (radiologist)
- 12. Follow-Up MRI to Monitor for ARIA in Patients Undergoing Treatment With an Anti-Amyloid Therapy (page 1 of 2) Patient Information Patient name:____________________________ Age:________ Sex:_______ Patient ID:___________________ Referring MD:___________________________________________ Purpose of scan (circle correct response): scheduled/asymptomatic monitoring for ARIA OR unscheduled/safety MRI in response to symptoms Report Information Scan Date:________________________________ Site Location:______________________________ Scan Information (fill in or circle response as needed) DWI Gadolinium Contrast ARIA–H Sequence ARIA–E Sequence Slice Gap Slice Thickness (mm) Field Strength Model Manufacturer Y N Y N SWI GRE/T2* 3D T2-FLAIR 1.5T 3T ARIA-E Summary Location (eg, frontal, parietal, occipital, temporal, brainstem, cerebellum) L/R Type (eg, parenchymal; sulcal) Change From Baseline (cm) Lesion Dynamics (eg, new, enlarging, shrinking, stable Max Diameter (cm) Lesion 1 Lesion 2 Lesion 3 Lesion 4 Treatment History Anti-Amyloid Agent: ________________________________ Number of doses received: ____________ Date of last dose: _______________________ Suspected ARIA Symptoms (if present): ______________________ Restricted Diffusion (circle correct response) Contrast Enhancement (circle correct response) Yes No N/A Yes No N/A
- 13. ARIA-H Summary Brainstem Deep Gray Cerebellum Temporal Frontal Parietal Occipital Total Current MCH count Baseline MCH count Change from baseline MCH count Current SS count Baseline SS count Change from baseline SS count Radiographic Severity (circle response) ARIA Type Severe Moderate Mild ≥1 location, >10 cm 1 location, 5-10 cm OR >1 location, each <10 cm 1 location, <5 cm ARIA-E ≥10 5-9 0-4 ARIA-H (MCH) >2 focal areas 2 focal areas 1 focal area ARIA-H (SS) Note other acute or chronic findings: _________________________________________________________________ _________________________________________________________________________________________________ Updated findings were conveyed to _____________________________ by _______________________________ (referring physician) (radiologist) Follow-Up MRI to Monitor for ARIA in Patients Undergoing Treatment With an Anti-Amyloid Therapy (page 2 of 2)
- 14. ARIA Standardized Reporting Template for PowerScribe Full abbreviations, accreditation, and disclosure information available at PeerView.com/MCV40 Download the XML code for a standardized and automated ARIA reporting template in PowerScribe by scanning the QR code or visiting the provided URL: www.PeerView.com/ARIA24-PowerScribeXML Once the file is downloaded, the code will need to be updated for your radiology department.